

Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis
- PMID: 17383982
- PMCID: PMC1852043
- DOI: 10.1136/bmj.39139.716794.55
Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis
Abstract
Objective: To review the literature on the use of inhaled nitric oxide to treat acute lung injury/acute respiratory distress syndrome (ALI/ARDS) and to summarise the effects of nitric oxide, compared with placebo or usual care without nitric oxide, in adults and children with ALI or ARDS.
Design: Systematic review and meta-analysis.
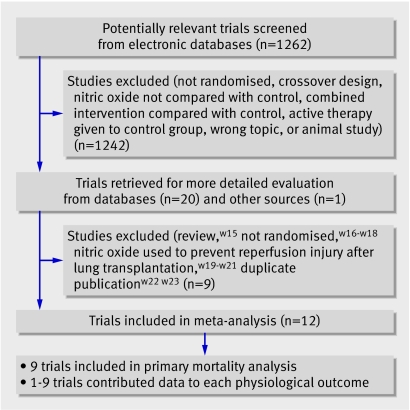
Data sources: Medline, CINAHL, Embase, and CENTRAL (to October 2006), proceedings from four conferences, and additional information from authors of 10 trials.
Review methods: Two reviewers independently selected parallel group randomised controlled trials comparing nitric oxide with control and extracted data related to study methods, clinical and physiological outcomes, and adverse events.
Main outcome measures: Mortality, duration of ventilation, oxygenation, pulmonary arterial pressure, adverse events.
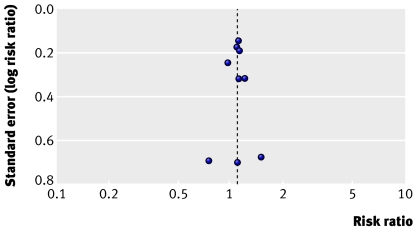
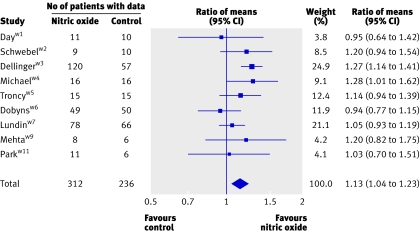
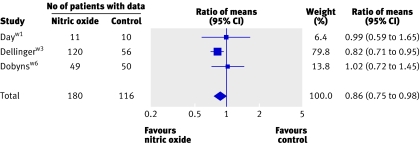
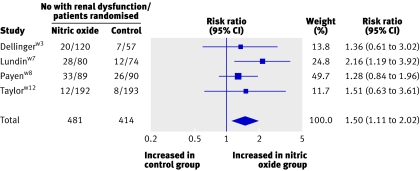
Results: 12 trials randomly assigning 1237 patients met inclusion criteria. Overall methodological quality was good. Using random effects models, we found no significant effect of nitric oxide on hospital mortality (risk ratio 1.10, 95% confidence interval 0.94 to 1.30), duration of ventilation, or ventilator-free days. On day one of treatment, nitric oxide increased the ratio of partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2 ratio) (13%, 4% to 23%) and decreased the oxygenation index (14%, 2% to 25%). Some evidence suggested that improvements in oxygenation persisted until day four. There was no effect on mean pulmonary arterial pressure. Patients receiving nitric oxide had an increased risk of developing renal dysfunction (1.50, 1.11 to 2.02).
Conclusions: Nitric oxide is associated with limited improvement in oxygenation in patients with ALI or ARDS but confers no mortality benefit and may cause harm. We do not recommend its routine use in these severely ill patients.
Conflict of interest statement
Figures

Comment in
-
Inhaled nitric oxide for acute respiratory distress syndrome.BMJ. 2007 Apr 14;334(7597):757-8. doi: 10.1136/bmj.39168.568692.BE. BMJ. 2007. PMID: 17431232 Free PMC article.
Similar articles
-
Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) and acute lung injury in children and adults.Cochrane Database Syst Rev. 2010 Jul 7;(7):CD002787. doi: 10.1002/14651858.CD002787.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2016 Jun 27;(6):CD002787. doi: 10.1002/14651858.CD002787.pub3. PMID: 20614430 Updated. Review.
-
The effect of inhaled nitric oxide in acute respiratory distress syndrome in children and adults: a Cochrane Systematic Review with trial sequential analysis.Anaesthesia. 2017 Jan;72(1):106-117. doi: 10.1111/anae.13628. Epub 2016 Oct 20. Anaesthesia. 2017. PMID: 27762438
-
Inhaled nitric oxide for acute respiratory distress syndrome and acute lung injury in adults and children: a systematic review with meta-analysis and trial sequential analysis.Anesth Analg. 2011 Jun;112(6):1411-21. doi: 10.1213/ANE.0b013e31820bd185. Epub 2011 Mar 3. Anesth Analg. 2011. PMID: 21372277 Review.
-
Inhaled nitric oxide does not reduce mortality in patients with acute respiratory distress syndrome regardless of severity: systematic review and meta-analysis.Crit Care Med. 2014 Feb;42(2):404-12. doi: 10.1097/CCM.0b013e3182a27909. Crit Care Med. 2014. PMID: 24132038 Review.
-
Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults.Cochrane Database Syst Rev. 2016 Jun 27;2016(6):CD002787. doi: 10.1002/14651858.CD002787.pub3. Cochrane Database Syst Rev. 2016. PMID: 27347773 Free PMC article. Review.
Cited by
-
Pharmacological interventions in acute respiratory distress syndrome.Ann Intensive Care. 2013 Jul 3;3(1):20. doi: 10.1186/2110-5820-3-20. Ann Intensive Care. 2013. PMID: 23822630 Free PMC article.
-
Extracorporeal support for trauma: A trauma quality improvement project (TQIP) analysis in patients with acute respiratory distress syndrome.Am J Emerg Med. 2021 Oct;48:170-176. doi: 10.1016/j.ajem.2021.04.083. Epub 2021 Apr 30. Am J Emerg Med. 2021. PMID: 33962131 Free PMC article.
-
A review of the use of inhaled nitric oxide in the PICU at Red Cross War Memorial Children's Hospital, 2011-2015: A retrospective cohort study.South Afr J Crit Care. 2021 Aug 6;37(2):10.7196/SAJCC.2021.v37i2.416. doi: 10.7196/SAJCC.2021.v37i2.416. eCollection 2021. South Afr J Crit Care. 2021. PMID: 35493980 Free PMC article.
-
Initial clinical impact of inhaled nitric oxide therapy for refractory hypoxemia following type A acute aortic dissection surgery.J Thorac Dis. 2019 Feb;11(2):495-504. doi: 10.21037/jtd.2019.01.42. J Thorac Dis. 2019. PMID: 30962993 Free PMC article.
-
H1N1-associated acute respiratory distress syndrome.Am J Med Sci. 2010 Dec;340(6):499-504. doi: 10.1097/MAJ.0b013e3181d94fa5. Am J Med Sci. 2010. PMID: 21119333 Free PMC article.
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149:819-24. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000;342:1334-49. - PubMed
-
- Furchgott RF. The 1996 Albert Lasker Medical Research Awards. The discovery of endothelium-derived relaxing factor and its importance in the identification of nitric oxide. JAMA 1996;276:1186-8. - PubMed
-
- Gries A, Bode C, Peter K, Herr A, Bohrer H, Motsch J, et al. Inhaled nitric oxide inhibits human platelet aggregation, P-selectin expression, and fibrinogen binding in vitro and in vivo. Circulation 1998;97:1481-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous