

X-Linked Hypophosphatemic Rickets: Multisystemic Disorder in Children Requiring Multidisciplinary Management
- PMID: 34421819
- PMCID: PMC8378329
- DOI: 10.3389/fendo.2021.688309
X-Linked Hypophosphatemic Rickets: Multisystemic Disorder in Children Requiring Multidisciplinary Management
Abstract
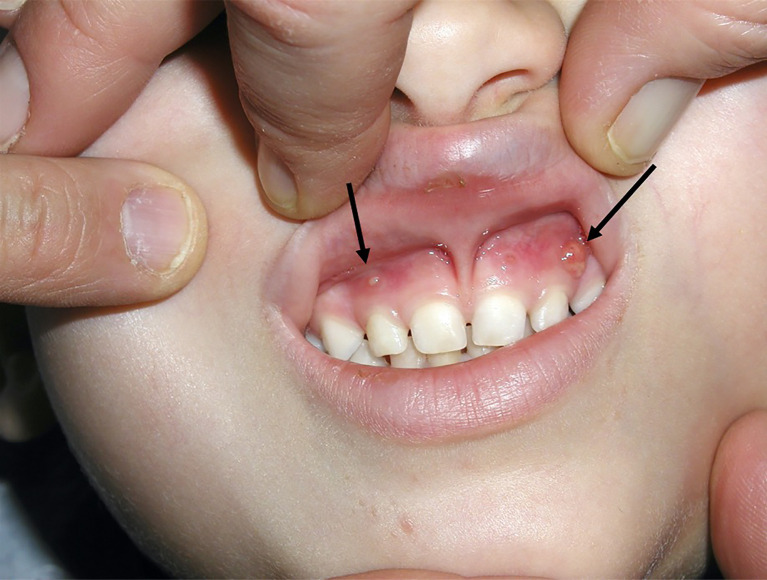
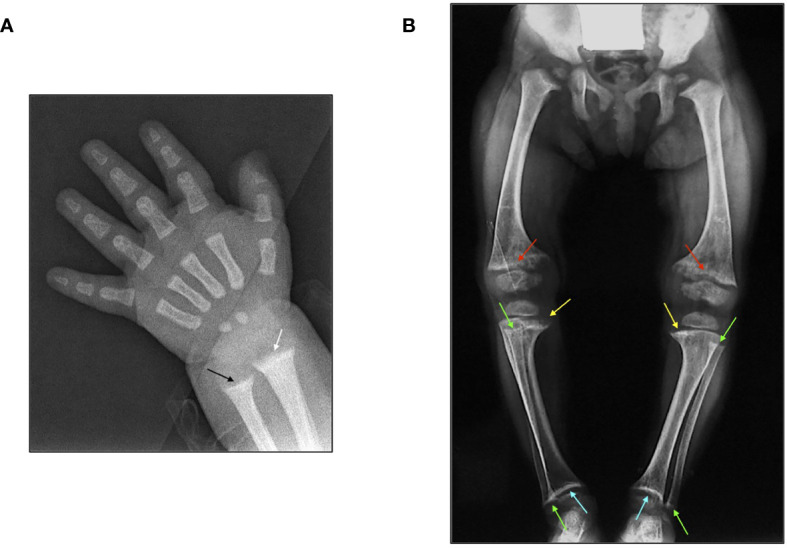
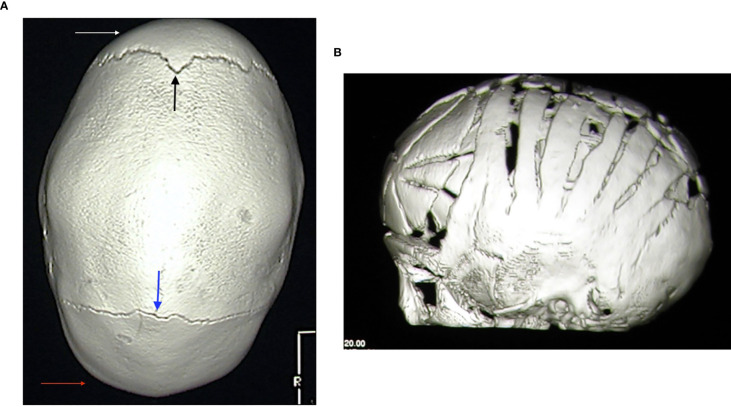
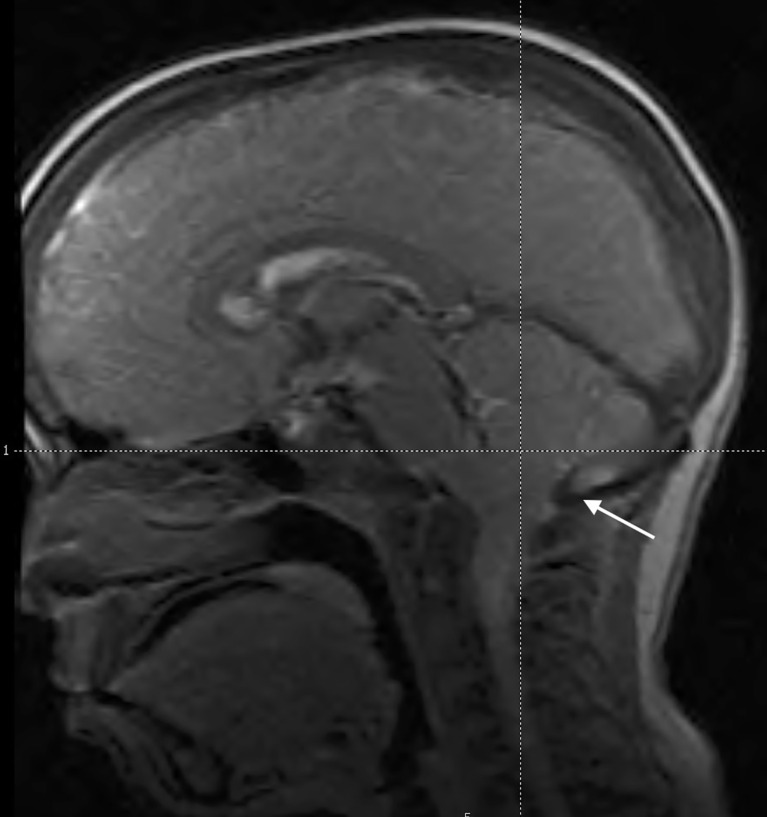
X-linked hypophosphatemic rickets (XLH) is the commonest inherited form of rickets. It is caused by an impaired regulation of fibroblast growth factor 23 (FGF23) due to a PHEX gene mutation, which leads to reduced tubular reabsorption of phosphate and renal 1α-hydroxylase activity and increased renal 24-hydroxylase activity. Hypophosphatemia associated with renal phosphate wasting, normal serum levels of calcium, parathyroid hormone, and 25-hydroxyvitamin D represents the main biochemical sign in affected patients. Patients with XLH show rickets and osteomalacia, severe deformities of the lower limbs, bone and muscular pain, stunted growth, and reduced quality of life. However, XLH is a multisystemic disorder requiring multidisciplinary approaches in specialized subdisciplines. Severe complications may occur in patients with XLH including craniosynostosis, hearing loss, progressive bone deformities, dental and periodontal recurrent lesions, and psychosocial distress. Moreover, long-term conventional treatment with active vitamin D metabolites and oral inorganic phosphate salts may cause endocrinological complications such as secondary or tertiary hyperparathyroidism, and adverse events in kidney as hypercalciuria, nephrocalcinosis, and nephrolithiasis. However, conventional treatment does not improve phosphate metabolism and it shows poor and slow effects in improving rickets lesions and linear growth. Recently, some trials of treatment with recombinant human IgG1 monoclonal antibody that targets FGF23 (burosumab) showed significant improvement of serum phosphate concentration and renal tubular reabsorption of phosphate that were associated with a rapid healing of radiologic signs of rickets, reduced muscular and osteoarticular pain, and improved physical function, being more effective for the treatment of patients with XLH in comparison with conventional therapy. Therefore, a global management of patients with XLH is strongly recommended and patients should be seen regularly by a multidisciplinary team of experts.
Keywords: X-linked hypophosphatemic rickets; burosumab; complication; conventional treatment; management.
Copyright © 2021 Baroncelli and Mora.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Safety and efficacy of burosumab in improving phosphate metabolism, bone health, and quality of life in adolescents with X-linked hypophosphatemic rickets.Eur J Med Genet. 2024 Aug;70:104958. doi: 10.1016/j.ejmg.2024.104958. Epub 2024 Jun 29. Eur J Med Genet. 2024. PMID: 38950880
-
Diagnosis and management of X-linked hypophosphatemia in children and adolescent in the Gulf Cooperation Council countries.Arch Osteoporos. 2021 Mar 4;16(1):52. doi: 10.1007/s11657-021-00879-9. Arch Osteoporos. 2021. PMID: 33660084 Free PMC article.
-
Rickets guidance: part II-management.Pediatr Nephrol. 2022 Oct;37(10):2289-2302. doi: 10.1007/s00467-022-05505-5. Epub 2022 Mar 29. Pediatr Nephrol. 2022. PMID: 35352187 Free PMC article.
-
FGF23 and Associated Disorders of Phosphate Wasting.Pediatr Endocrinol Rev. 2019 Sep;17(1):17-34. doi: 10.17458/per.vol17.2019.gi.fgf23anddisordersphosphate. Pediatr Endocrinol Rev. 2019. PMID: 31599133 Free PMC article. Review.
-
Consensus Recommendations for the Diagnosis and Management of X-Linked Hypophosphatemia in Belgium.Front Endocrinol (Lausanne). 2021 Mar 19;12:641543. doi: 10.3389/fendo.2021.641543. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33815294 Free PMC article. Review.
Cited by
-
Bone Turnover Markers and Bone Mineral Density in Children with Hypophosphatemic Rickets.J Clin Med. 2022 Aug 8;11(15):4622. doi: 10.3390/jcm11154622. J Clin Med. 2022. PMID: 35956239 Free PMC article.
-
Current and Future Therapeutical Aspects of X-Linked Hypophosphatemia in Children With Special Attention to Klotho/Fibroblast Growth Factor 23 System.J Clin Med Res. 2022 Oct;14(10):436-439. doi: 10.14740/jocmr4820. Epub 2022 Oct 28. J Clin Med Res. 2022. PMID: 36406946 Free PMC article. No abstract available.
-
[Advances in the study of fluctuating sensorineural hearing loss].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Mar;37(3):238-242. doi: 10.13201/j.issn.2096-7993.2023.03.017. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 36843527 Free PMC article. Review. Chinese.
-
Alkaline phosphatase in clinical practice in childhood: Focus on rickets.Front Endocrinol (Lausanne). 2023 Feb 2;14:1111445. doi: 10.3389/fendo.2023.1111445. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 36817604 Free PMC article. Review.
-
Temporary hemiepiphysiodesis using eight-plates for angular deformities of the lower extremities in children with X-linked hypophosphataemic rickets.Int Orthop. 2023 Mar;47(3):763-771. doi: 10.1007/s00264-023-05688-y. Epub 2023 Jan 16. Int Orthop. 2023. PMID: 36646902 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources