

Safety and tolerability of inebilizumab (MEDI-551), an anti-CD19 monoclonal antibody, in patients with relapsing forms of multiple sclerosis: Results from a phase 1 randomised, placebo-controlled, escalating intravenous and subcutaneous dose study
- PMID: 29143550
- PMCID: PMC6360486
- DOI: 10.1177/1352458517740641
Safety and tolerability of inebilizumab (MEDI-551), an anti-CD19 monoclonal antibody, in patients with relapsing forms of multiple sclerosis: Results from a phase 1 randomised, placebo-controlled, escalating intravenous and subcutaneous dose study
Abstract
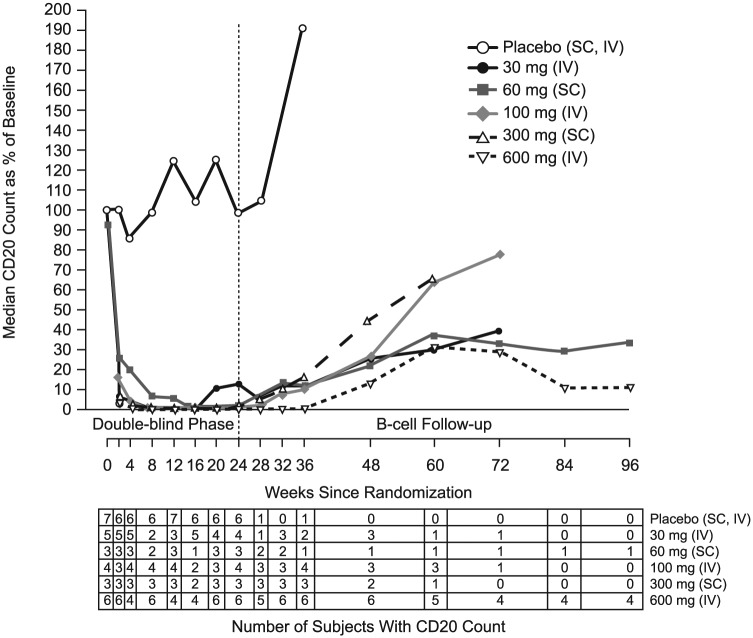
Background: B cells may be involved in the pathophysiology of multiple sclerosis (MS). Inebilizumab (formerly MEDI-551) binds to and depletes CD19+ B cells.
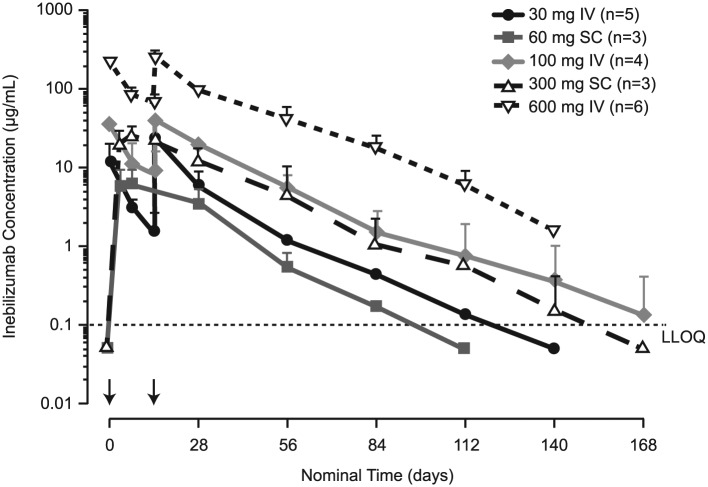
Objectives: To assess safety, tolerability, pharmacokinetics, pharmacodynamics and immunogenicity of inebilizumab in adults with relapsing MS.
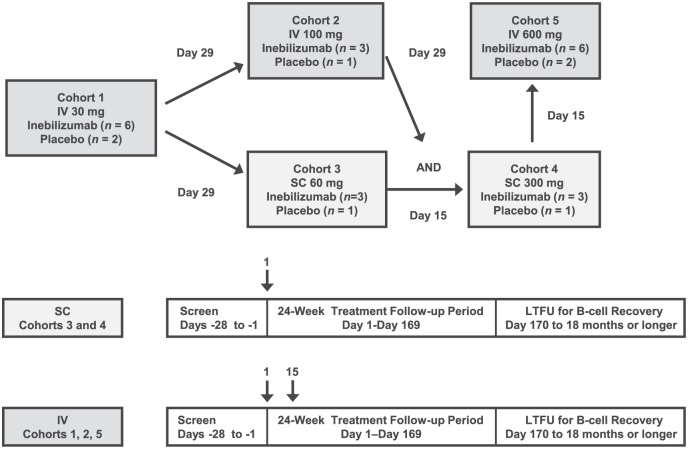
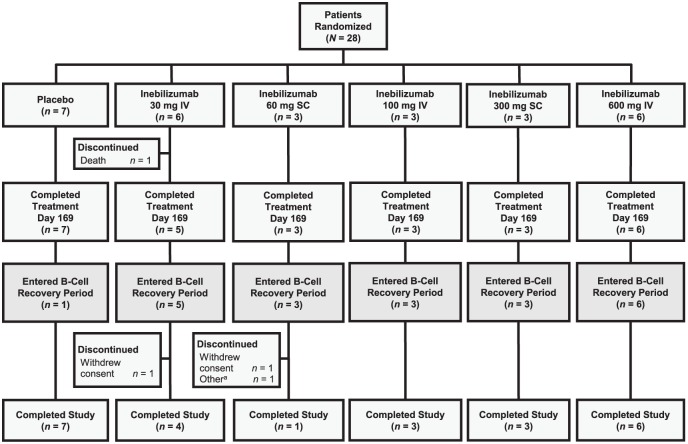
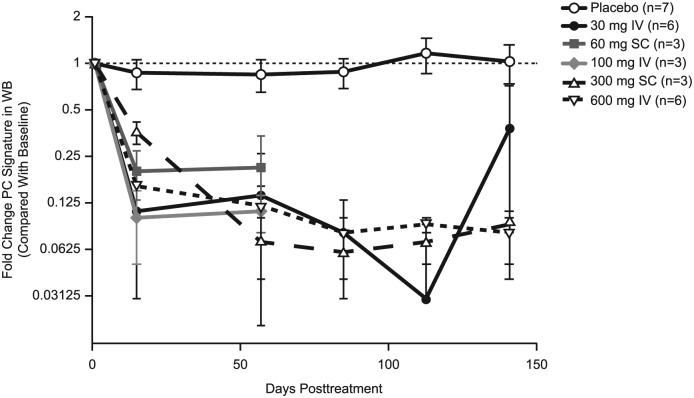
Methods: This phase 1 trial randomised 28 patients 3:1 (21, inebilizumab; 7, placebo) to inebilizumab (2 intravenous (IV) doses, days 1 and 15: 30, 100 or 600 mg; or single subcutaneous (SC) dose on day 1: 60 or 300 mg) or matching placebo, with follow-up until at least week 24 or return of CD19+ B-cell count to ⩾80 cells/µL.
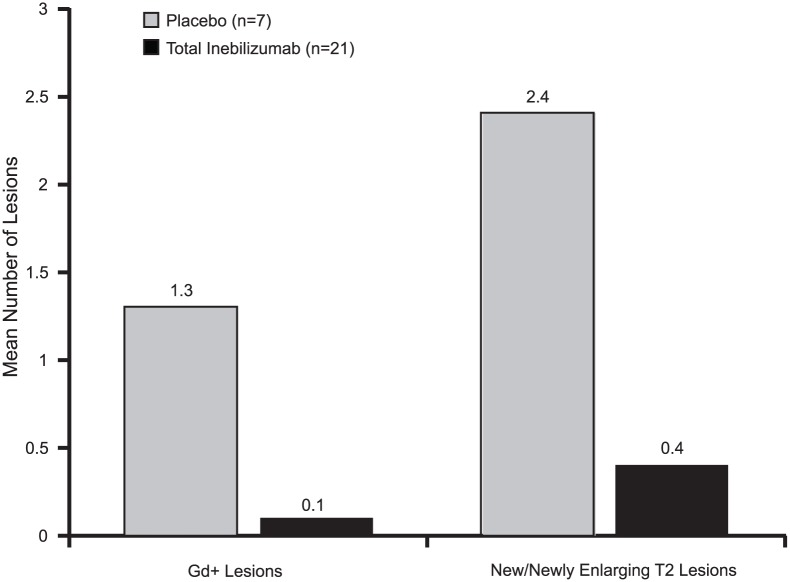
Results: Complete B-cell depletion was observed across all doses. Infusion/injection (grade 1/2) reactions occurred in 6/15 patients receiving inebilizumab IV, 2/5 placebo IV and 1/6 inebilizumab SC. Serious adverse events occurred in three patients receiving inebilizumab: pyrexia, mixed-drug intoxication (unrelated to inebilizumab; resulted in death) and urinary tract infection. Mean number of cumulative new gadolinium-enhancing lesions over 24 weeks was 0.1 with inebilizumab versus 1.3 with placebo; mean numbers of new/newly enlarging T2 lesions were 0.4 and 2.4, respectively.
Conclusion: Inebilizumab had an acceptable safety profile in relapsing MS patients and showed a trend in reductions in new/newly enlarging and gadolinium-enhancing lesions.
Keywords: B cells; intravenous administration; pharmacodynamics; pharmacokinetics; subcutaneous administration.
Conflict of interest statement
Figures
Similar articles
-
Safety and tolerability of an anti-CD19 monoclonal antibody, MEDI-551, in subjects with systemic sclerosis: a phase I, randomized, placebo-controlled, escalating single-dose study.Arthritis Res Ther. 2016 Jun 7;18(1):131. doi: 10.1186/s13075-016-1021-2. Arthritis Res Ther. 2016. PMID: 27267753 Free PMC article. Clinical Trial.
-
Inebilizumab for the treatment of neuromyelitis optica spectrum disorder (N-MOmentum): a double-blind, randomised placebo-controlled phase 2/3 trial.Lancet. 2019 Oct 12;394(10206):1352-1363. doi: 10.1016/S0140-6736(19)31817-3. Epub 2019 Sep 5. Lancet. 2019. PMID: 31495497 Clinical Trial.
-
Ocrelizumab in relapsing-remitting multiple sclerosis: a phase 2, randomised, placebo-controlled, multicentre trial.Lancet. 2011 Nov 19;378(9805):1779-87. doi: 10.1016/S0140-6736(11)61649-8. Epub 2011 Oct 31. Lancet. 2011. PMID: 22047971 Clinical Trial.
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
Natalizumab for relapsing remitting multiple sclerosis.Cochrane Database Syst Rev. 2011 Oct 5;(10):CD007621. doi: 10.1002/14651858.CD007621.pub2. Cochrane Database Syst Rev. 2011. PMID: 21975773 Review.
Cited by
-
Drug Treatment of Neuromyelitis Optica Spectrum Disorders: Out with the Old, in with the New?Immunotargets Ther. 2021 Mar 19;10:87-101. doi: 10.2147/ITT.S287652. eCollection 2021. Immunotargets Ther. 2021. PMID: 33777853 Free PMC article. Review.
-
Targeting B cells and plasma cells in autoimmune diseases: From established treatments to novel therapeutic approaches.Eur J Immunol. 2023 Jan;53(1):e2149675. doi: 10.1002/eji.202149675. Epub 2022 Nov 16. Eur J Immunol. 2023. PMID: 36314264 Free PMC article. Review.
-
Monoclonal antibody and protein therapeutic formulations for subcutaneous delivery: high-concentration, low-volume vs. low-concentration, high-volume.MAbs. 2023 Jan-Dec;15(1):2285277. doi: 10.1080/19420862.2023.2285277. Epub 2023 Nov 27. MAbs. 2023. PMID: 38013454 Free PMC article. Review.
-
Recent progress in maintenance treatment of neuromyelitis optica spectrum disorder.J Neurol. 2021 Dec;268(12):4522-4536. doi: 10.1007/s00415-020-10235-5. Epub 2020 Oct 3. J Neurol. 2021. PMID: 33011853 Free PMC article. Review.
-
The Role of B Cells and B Cell Therapies in Immune-Mediated Liver Diseases.Front Immunol. 2021 Apr 14;12:661196. doi: 10.3389/fimmu.2021.661196. eCollection 2021. Front Immunol. 2021. PMID: 33936097 Free PMC article. Review.
References
-
- Baranzini SE, Jeong MC, Butunoi C, et al. B cell repertoire diversity and clonal expansion in multiple sclerosis brain lesions. J Immunol 1999; 163: 5133–5144. - PubMed
-
- Duddy M, Niino M, Adatia F, et al. Distinct effector cytokine profiles of memory and naive human B cell subsets and implication in multiple sclerosis. J Immunol 2007; 178: 6092–6099. - PubMed
-
- Faissner S, Nikolayczik J, Chan A, et al. Plasmapheresis and immunoadsorption in patients with steroid refractory multiple sclerosis relapses. J Neurol 2016; 263: 1092–1098. - PubMed
-
- Knippenberg S, Peelen E, Smolders J, et al. Reduction in IL-10 producing B cells (Breg) in multiple sclerosis is accompanied by a reduced naive/memory Breg ratio during a relapse but not in remission. J Neuroimmunol 2011; 239: 80–86. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
