

Fibrodysplasia ossificans progressiva: diagnosis, management, and therapeutic horizons
- PMID: 23858627
- PMCID: PMC3995352
Fibrodysplasia ossificans progressiva: diagnosis, management, and therapeutic horizons
Abstract
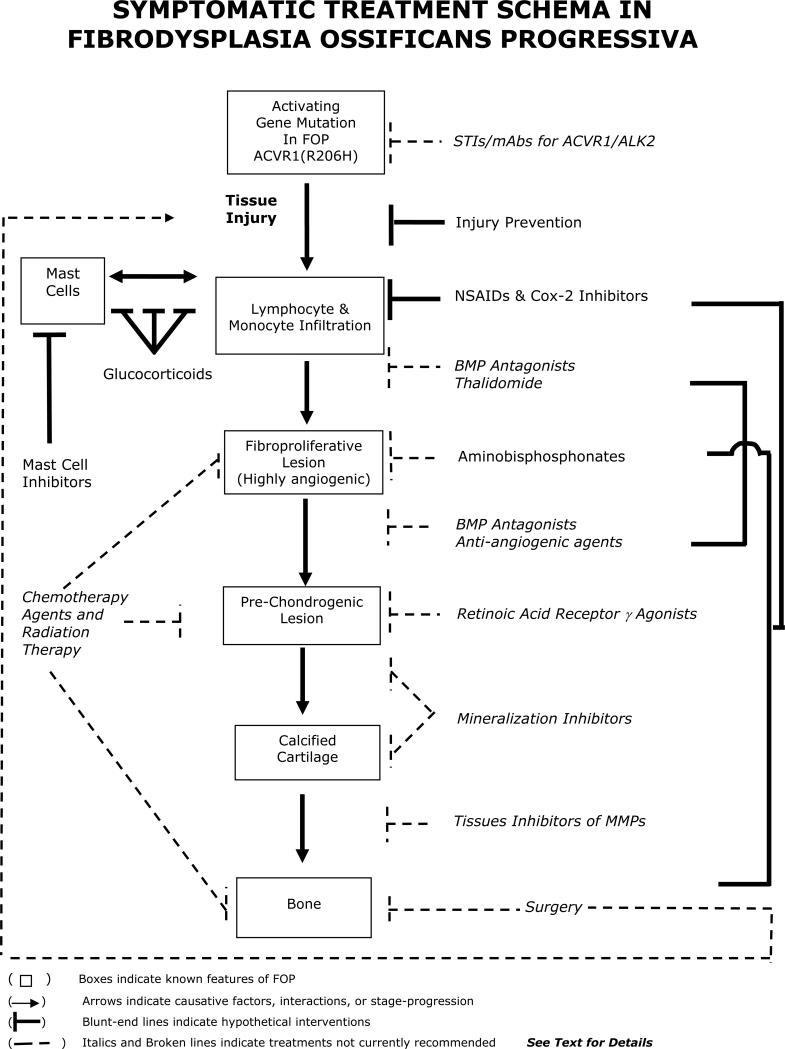
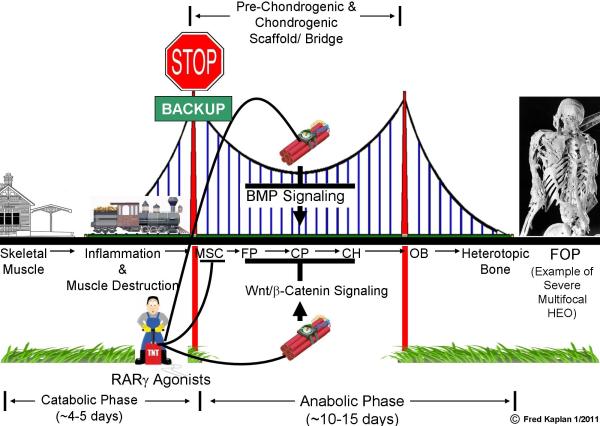
Fibrodysplasia ossificans progressiva (FOP), a rare and disabling genetic condition characterized by congenital malformations of the great toes and progressive heterotopic endochondral ossification (HEO) which is the most catastrophic of HEO disorders in humans. Flare-ups of FOP are episodic; immobility is cumulative. Heterozygous activating mutations in activin receptor IA/activin-like kinase-2 (ACVRI/ ALK2), a bone morphogenetic protein (BMP) type I receptor, exist in all sporadic and familial cases of FOP. The discovery of the FOP gene established a critical milestone in our understanding of FOP, and revealed a highly conserved therapeutic target in the BMP signaling pathway. This discovery has advanced efforts to develop novel therapies for this disabling disorder of tissue metamorphosis. While effective treatment of FOP will likely be based on interventions that modulate overactive ACVR1/ALK2 signaling, or that specifically block postnatal HEO, current management is focused on early diagnosis, assiduous avoidance of injury or iatrogenic harm, symptomatic amelioration of painful flare-ups, and optimization of residual function.
Figures

Similar articles
-
Fibrodysplasia ossificans progressiva.Best Pract Res Clin Rheumatol. 2008 Mar;22(1):191-205. doi: 10.1016/j.berh.2007.11.007. Best Pract Res Clin Rheumatol. 2008. PMID: 18328989 Free PMC article. Review.
-
Fibrodysplasia ossificans progressiva: a blueprint for metamorphosis.Ann N Y Acad Sci. 2011 Nov;1237:5-10. doi: 10.1111/j.1749-6632.2011.06195.x. Ann N Y Acad Sci. 2011. PMID: 22082359 Free PMC article. Review.
-
Fibrodysplasia ossificans progressiva: clinical and genetic aspects.Orphanet J Rare Dis. 2011 Dec 1;6:80. doi: 10.1186/1750-1172-6-80. Orphanet J Rare Dis. 2011. PMID: 22133093 Free PMC article. Review.
-
International physician survey on management of FOP: a modified Delphi study.Orphanet J Rare Dis. 2017 Jun 12;12(1):110. doi: 10.1186/s13023-017-0659-4. Orphanet J Rare Dis. 2017. PMID: 28606101 Free PMC article.
-
Granting immunity to FOP and catching heterotopic ossification in the Act.Semin Cell Dev Biol. 2016 Jan;49:30-6. doi: 10.1016/j.semcdb.2015.12.013. Epub 2015 Dec 17. Semin Cell Dev Biol. 2016. PMID: 26706149 Free PMC article. Review.
Cited by
-
Clinical Aspects and Current Therapeutic Approaches for FOP.Biomedicines. 2020 Sep 2;8(9):325. doi: 10.3390/biomedicines8090325. Biomedicines. 2020. PMID: 32887348 Free PMC article. Review.
-
The presentation, assessment, pathogenesis, and treatment of calcinosis in juvenile dermatomyositis.Curr Rheumatol Rep. 2014 Dec;16(12):467. doi: 10.1007/s11926-014-0467-y. Curr Rheumatol Rep. 2014. PMID: 25366934 Free PMC article. Review.
-
Human osteoarthritis cartilage-derived stromal cells activate joint degeneration through TGF-beta lateral signaling.FASEB J. 2020 Dec;34(12):16552-16566. doi: 10.1096/fj.202001448R. Epub 2020 Oct 29. FASEB J. 2020. PMID: 33118211 Free PMC article.
-
Fibrodysplasia ossificans progressiva: current concepts from bench to bedside.Dis Model Mech. 2020 Sep 21;13(9):dmm046441. doi: 10.1242/dmm.046441. Dis Model Mech. 2020. PMID: 32988985 Free PMC article. Review.
-
A Rare Grotesque Skeletal Deformity: Munchmeyer's Disease.Mediterr J Rheumatol. 2021 Mar 31;32(1):91. doi: 10.31138/mjr.32.1.91. eCollection 2021 Mar. Mediterr J Rheumatol. 2021. PMID: 34386708 Free PMC article. No abstract available.
References
-
- Shore EM, Feldman GJ, Xu M, Kaplan FS. The genetics of fibrodysplasia ossificans progressiva. Clin Rev Bone Miner Metab. 2005;3:201–204.
-
- Cohen RB, Hahn GV, Tabas JA, Peeper J, Levitz CL, Sando A, Sando N, Zasloff M, Kaplan FS. The natural history of heterotopic ossification in patients who have fibrodysplasia ossificans progressiva. A study of forty-four patients. J Bone Joint Surg Am. 1993;75:215–219. - PubMed
-
- Rocke DM, Zasloff M, Peeper J, Cohen RB, Kaplan FS. Age- and joint-specific risk of initial heterotopic ossification in patients who have fibrodysplasia ossificans progressiva. Clin Orthop Relat Res. 1994:243–248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources