

Clinical, legal and ethical implications of coercion and compulsory treatment in eating disorders: do rapid review findings identify clear answers or more muddy waters?
- PMID: 39425146
- PMCID: PMC11490133
- DOI: 10.1186/s40337-024-01120-x
Clinical, legal and ethical implications of coercion and compulsory treatment in eating disorders: do rapid review findings identify clear answers or more muddy waters?
Abstract
Introduction: This Rapid Review (RR) aimed to assess the current literature over the past decade to determine the prevailing evidence regarding compulsory treatment* in eating disorders (ED). It is hoped that the review will help inform a consensus opinion as to whether this course of action confers significant clinical benefit, and importantly, to whom it should apply. The review also explores alternative options to involuntary care.
Methods: Four indexing databases (OVID; ProQuest; Web of Science; PubMed/MedLine) were searched using variations of the following keywords: "coercive/detained/involuntary/least restrictive care" "treatment refusal" "incarcerated/forced/compulsory admission" "moral/ethic/legal/mental health act" "eating disorder". Research was restricted to articles published between 2013 and 2023 and included grey literature.
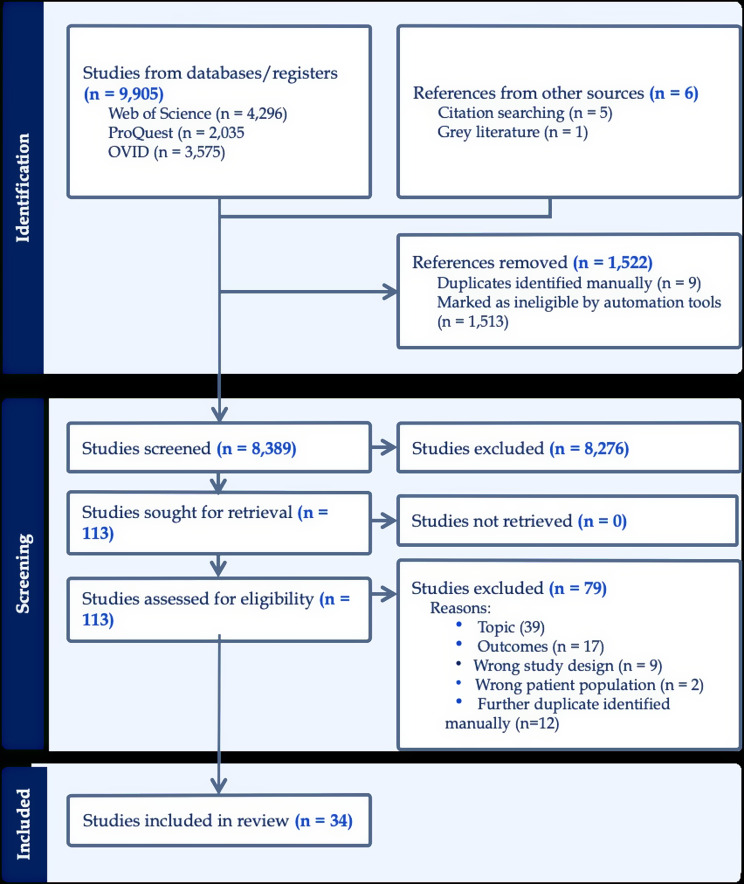
Results: Of 9911 articles retrieved, 34 were included for final analyses, exploring ethical, legal, and physical and mental health outcomes of compulsory treatment. Studies comprised review papers, cohort studies, cross sectional research, case series reports, ethnography, commentary papers and grey literature. The majority of studies focused on individuals with anorexia nervosa (AN). Only two papers considered compulsory treatment in individuals with other eating disorders (EDs) Findings largely align with previous reviews suggesting compulsory treatment saves lives but comes at a therapeutic and personal cost. It remains unknown as to who may benefit from compulsory treatment. The decision to invoke compulsory treatment remains with the clinician and is a responsibility that is likely to be faced by most in their care of individuals with EDs.
Conclusions: Significant gaps remain in the published literature and a clear road map for a clinician-informed decision on the submission of a compulsory treatment for a person with ED does not yet exist. Further, there is little evidence as to who is most likely to benefit from compulsory treatment. There is consensus that efforts should be concentrated on reducing instances of compulsory treatment and minimising coercion through the development of open, transparent and trusting relationships between individuals and their treating clinician. Co-produced research and the development of clinical guidelines guided by the voices of individuals with lived experience are needed to ensure minimisation of potential harm.
Keywords: Anorexia nervosa; Coercive; Compulsory treatment; Detained; Eating disorder; Ethics; Iatrogenic; Inpatient; Involuntary; Involuntary treatment; Mental health act.
Plain language summary
Eating disorders are complex psychological disorders with numerous significant physical health consequences associated with lethality including heart attack, irregular heartbeat, dehydration, blood clots, and risk of suicide. Without indicated intervention for physical deterioration in the acute stages of illness, individuals are likely at best to develop a chronic course and at worst to lose their life. Despite this, individuals frequently refuse intervention and medical treatment due to fear of weight gain, the interruption of behaviours that are experienced as protective and the effects of past experiences of care. Many report a sense of hopelessness and fear due to past unsuccessful and at times harmful treatments. This presents treating clinicians with a practical and ethical conundrum: should treatment be delivered to an individual against their will? Researchers, policymakers, law professionals and lived experience alike are challenged as to the legal and ethical bounds around which practitioners can act with beneficence when considering compulsory treatment of an individual with an eating disorder. A Rapid Review was commissioned by the Victorian Government Department of Health to summarise the extant literature on the compulsory treatment* of individuals with eating disorders. * Involuntary treatment’ and ‘compulsory treatment’ are synonymous, but we have chosen the term that is best understood by the general public/informed readers.
© 2024. The Author(s).
Conflict of interest statement
P.H. receives sessional fees and lecture fees from the Australian Medical Council, Therapeutic Guidelines publication, and HETI, and royalties from Hogrefe and Huber, McGraw Hill Education, and Blackwell Scientific Publications, and she has received research grants from the NHMRC and ARC. She is Chair of the National Eating Disorders Collaboration Steering Committee in Australia and was a Member of the ICD-11 Working Group for Eating Disorders and was Chair Clinical Practice Guidelines Project Working Group (Eating Disorders) of RANZCP. She has been a consultant to Takeda Pharmaceuticals. All views in this paper are her own. S.T. receives royalties from Taylor and Francis, Hogrefe and Huber and McGraw Hill for published book chapters. He has received honoraria from Shire/ Takeda Group of Companies for chairing the Australian Clinical Advisory Board for Binge Eating Disorder, public speaking engagements, commissioned reports as well as investigator- initiated research grants. He is an Editor in Chief of this journal, an inaugural committee member of the National Eating Disorders Collaboration, a Member of the Technical Advisory Group (TAG) on Eating Disorders (Commonwealth of Australia) and a member of the governing council of the Australian Eating Disorders Research and Translation Centre. J.Y. is section editor (Eating Disorders) for UpToDate published by Wolters Kluwer. The other authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Indications for involuntary hospitalization for refusal of treatment in severe anorexia nervosa: a survey of physicians and mental health care review board members in Japan.J Eat Disord. 2022 Nov 21;10(1):176. doi: 10.1186/s40337-022-00703-w. J Eat Disord. 2022. PMID: 36415005 Free PMC article.
-
Coercion and Compulsory Treatment in Anorexia Nervosa: a Systematic Review on Legal and Ethical Issues.Psychiatr Danub. 2023 Oct;35(Suppl 2):206-216. Psychiatr Danub. 2023. PMID: 37800229
-
Compulsory treatments in eating disorders: a systematic review and meta-analysis.Eat Weight Disord. 2021 May;26(4):1037-1048. doi: 10.1007/s40519-020-01031-1. Epub 2020 Oct 24. Eat Weight Disord. 2021. PMID: 33099675 Free PMC article. Review.
-
Involuntary admission: the case of anorexia nervosa.Int J Law Psychiatry. 2015 Mar-Apr;39:31-5. doi: 10.1016/j.ijlp.2015.01.018. Epub 2015 Feb 7. Int J Law Psychiatry. 2015. PMID: 25660351 Review.
References
-
- Yager J. Managing patients with severe and enduring Anorexia Nervosa: when is enough. Enough? J Nerv Ment Dis. 2020;208(4):277–82. - PubMed
-
- Elzakkers IFFM, Danner UN, Hoek HW, Schmidt U, Van Elburg AA. Compulsory treatment in anorexia nervosa: a review. Intl J Eat Disorders. 2014;47(8):845–52. - PubMed
-
- Papadopoulos FC, Ekbom A, Brandt L, Ekselius L. Excess mortality, causes of death and prognostic factors in anorexia nervosa. Br J Psychiatry. 2009;194(1):10–7. - PubMed
-
- Touyz S, Carney AOT. Compulsory (involuntary) treatment for anorexia nervosa. In: Grilo C, Mitchell J, editors. The treatment of eating disorders. Guilford Press, 2010. p. 212–224. Sydney Law School Research Paper No. 10/07, Available at SSRN: https://ssrn.com/abstract=1531975
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
