

A Heterozygous Phospholamban Variant (p.R14del) Leads to Left Ventricular Involvement and Heart Failure Phenotypes in Arrhythmogenic Right Ventricular Cardiomyopathy
- PMID: 38605909
- PMCID: PMC11003943
- DOI: 10.1007/s43657-023-00126-w
A Heterozygous Phospholamban Variant (p.R14del) Leads to Left Ventricular Involvement and Heart Failure Phenotypes in Arrhythmogenic Right Ventricular Cardiomyopathy
Abstract
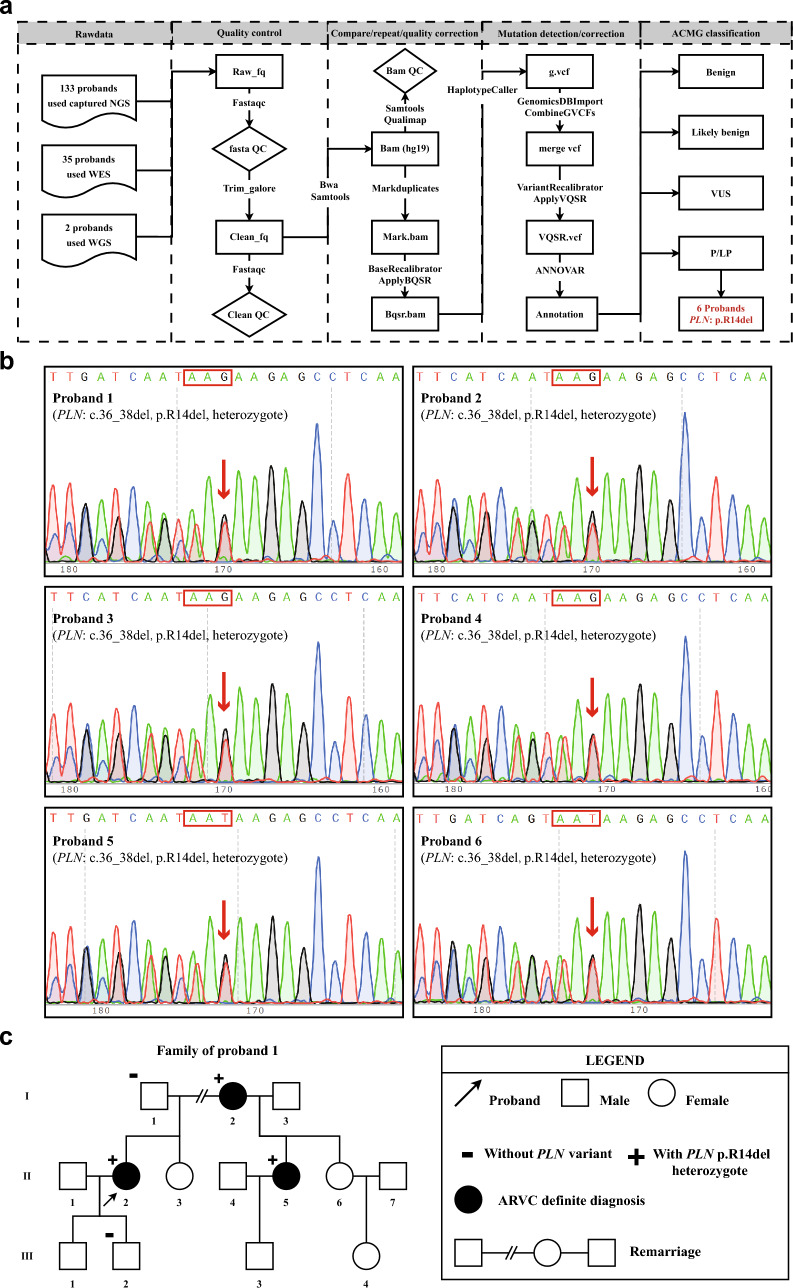
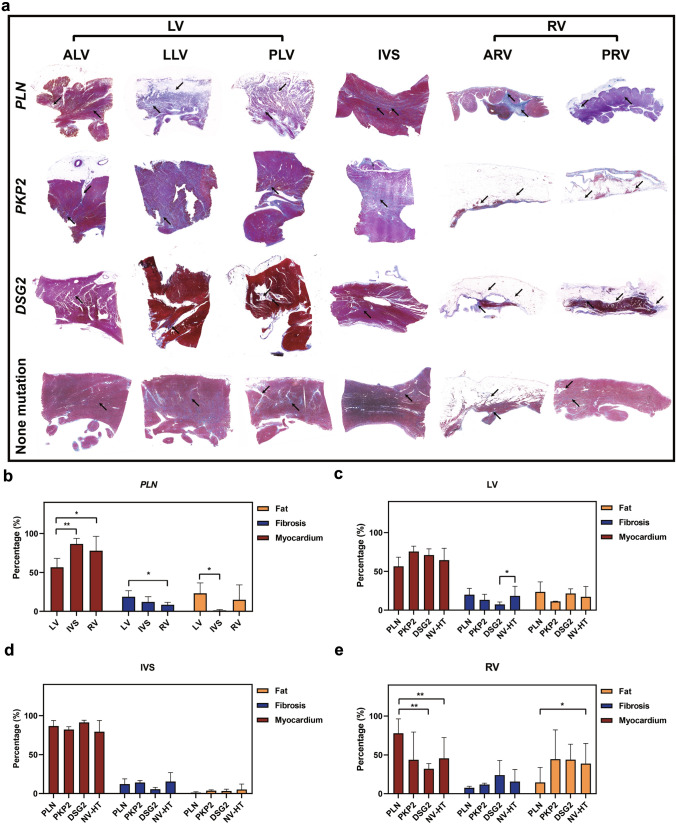
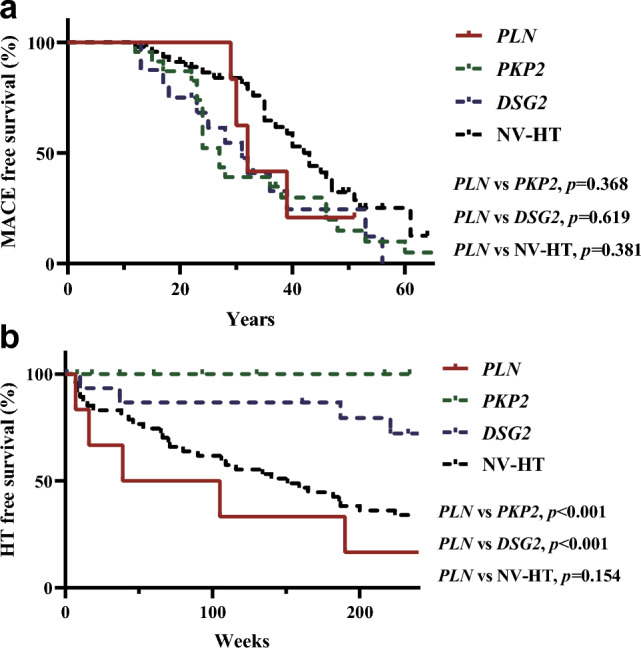
This study aimed to determine the prevalence and clinical features of Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) caused by pathogenic mutations in the Phospholamban (PLN) gene. The study included 170 patients who had a confirmed diagnosis of ARVC and underwent PLN genetic screening using next-generation sequencing. The findings of this study provide valuable insights into the association between PLN mutations and ARVC, which can aid in the development of more effective diagnostic and treatment strategies for ARVC patients. Out of the patients evaluated, six had a rare pathogenic mutation in PLN with the same p.R14del variant. Family screening revealed that heterozygous carriers of p.R14del exhibited a definite ARVC phenotype. In clinical studies, individuals with the p.R14del mutation experienced a similar rate of malignant arrhythmia events as those with classic desmosome mutations. After adjusting for covariates, individuals with PLN mutations had a two point one seven times greater likelihood of experiencing transplant-related risks compared to those who did not possess PLN mutations (95% CI 1.08-6.82, p = 0.035). The accumulation of left ventricular fat and fibers is a pathological marker for ARVC patients with p.R14del mutations. In a cohort of 170 Chinese ARVC patients, three point five percent of probands had the PLN pathogenic variant (p.R14del) and all were female. Our data shows that PLN-related ARVC patients are at high risk for ventricular arrhythmias and heart failure, which requires clinical differentiation from classic ARVC. Furthermore, carrying the p.R14del mutation can be an independent prognostic risk factor in ARVC patients.
Supplementary information: The online version contains supplementary material available at 10.1007/s43657-023-00126-w.
Keywords: Arrhythmogenic right ventricular cardiomyopathy; Heart failure; Left ventricular involvement; Phospholamban; Risk stratification.
© International Human Phenome Institutes (Shanghai) 2024. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestThe authors have no conflicts of interest to declare in relation to this study.
Figures
Similar articles
-
Can a Liquid Biopsy Detect Circulating Tumor DNA With Low-passage Whole-genome Sequencing in Patients With a Sarcoma? A Pilot Evaluation.Clin Orthop Relat Res. 2025 Jan 1;483(1):39-48. doi: 10.1097/CORR.0000000000003161. Epub 2024 Jun 21. Clin Orthop Relat Res. 2025. PMID: 38905450
-
Defining the optimum strategy for identifying adults and children with coeliac disease: systematic review and economic modelling.Health Technol Assess. 2022 Oct;26(44):1-310. doi: 10.3310/ZUCE8371. Health Technol Assess. 2022. PMID: 36321689 Free PMC article.
-
Reduced plakoglobin increases the risk of sodium current defects and atrial conduction abnormalities in response to androgenic anabolic steroid abuse.J Physiol. 2024 Sep;602(18):4409-4436. doi: 10.1113/JP284597. Epub 2024 Feb 12. J Physiol. 2024. PMID: 38345865
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article. Review.
-
Pharmacological and non-pharmacological treatments and outcomes for new-onset atrial fibrillation in ICU patients: the CAFE scoping review and database analyses.Health Technol Assess. 2021 Nov;25(71):1-174. doi: 10.3310/hta25710. Health Technol Assess. 2021. PMID: 34847987
References
LinkOut - more resources
Full Text Sources