

Multiple vascular anomalies and refractory pericardial effusion in a young patient with Cantu syndrome: a case report and review of the literature
- PMID: 38114927
- PMCID: PMC10731865
- DOI: 10.1186/s12887-023-04446-8
Multiple vascular anomalies and refractory pericardial effusion in a young patient with Cantu syndrome: a case report and review of the literature
Abstract
Background: Cantu syndrome is a rare and complex multisystem disorder characterized by hypertrichosis, facial dysmorphism, osteochondroplasia and cardiac abnormalities. With only 150 cases reported worldwide, Cantu syndrome is now gaining wider recognition due to molecular testing and a growing body of literature that further characterizes the syndrome and some of its most important features. Cardiovascular pathology previously described in the literature include cardiomegaly, pericardial effusion, vascular dilation and tortuosity, and other congenital heart defects. However, cardiovascular involvement is highly variable amongst individuals with Cantu syndrome. In some instances, it can be extensive and severe requiring surgical management and long term follow up.
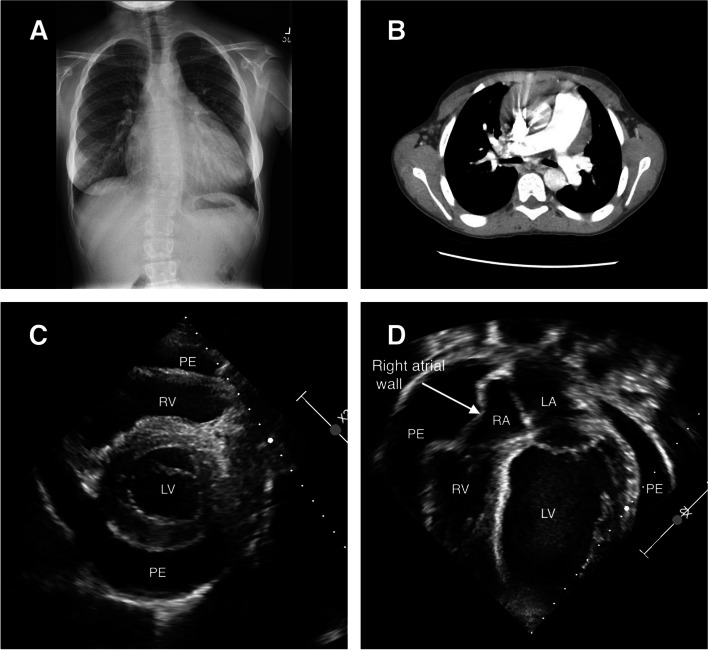
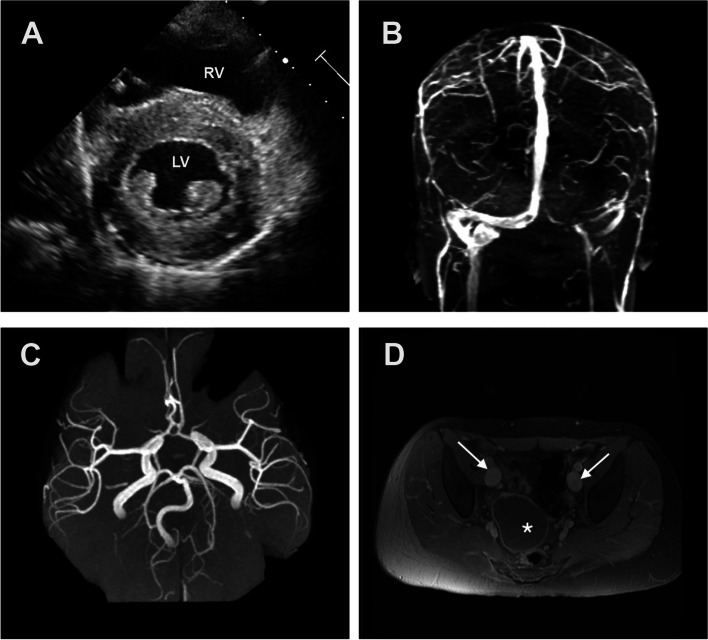
Case presentation: Herein we report a case of a fourteen-year-old female who presented with worsening pericardial effusion of unknown etiology, and echocardiographic findings of concentric left ventricular hypertrophy, a mildly dilated aortic root and ascending aorta. Her medical history was notable for hemoptysis and an episode of pulmonary hemorrhage secondary to multiple aortopulmonary collaterals that were subsequently embolized in early childhood. She was initially managed with Ibuprofen and Colchicine but continued to worsen, and ultimately required a pericardial window for the management of refractory pericardial effusion. Imaging studies obtained on subsequent visits revealed multiple dilated and tortuous blood vessels in the head, neck, chest, and pelvis. A cardiomyopathy molecular studies panel was sent, and a pathogenic variant was identified in the ABCC9 gene, confirming the molecular diagnosis of autosomal dominant Cantu syndrome.
Conclusions: Vascular anomalies and significant cardiac involvement are often present in Cantu syndrome, however there are currently no established screening recommendations or surveillance protocols in place. The triad of hypertrichosis, facial dysmorphism, and unexplained cardiovascular involvement in any patient should raise suspicion for Cantu syndrome and warrant further investigation. Initial cardiac evaluation and follow up should be indicated in any patient with a clinical and/or molecular diagnosis of Cantu syndrome. Furthermore, whole body imaging should be utilized to evaluate the extent of vascular involvement and dictate long term monitoring and care.
Keywords: ABCC9 gene; Aortic root dilation; Cantu syndrome; Cardiomegaly; Hypertrichosis; KCNJ8 gene; Left ventricular hypertrophy; Lymphedema; Pericardial effusion.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Cantu syndrome in a woman and her two daughters: Further confirmation of autosomal dominant inheritance and review of the cardiac manifestations.Am J Med Genet A. 2006 Aug 1;140(15):1673-80. doi: 10.1002/ajmg.a.31348. Am J Med Genet A. 2006. PMID: 16835932
-
Cantú syndrome as a rare cause of pericardial effusion in a young woman.Br J Hosp Med (Lond). 2019 Dec 2;80(12):732-733. doi: 10.12968/hmed.2019.80.12.732. Br J Hosp Med (Lond). 2019. PMID: 31822179 No abstract available.
-
Cantu syndrome: A longitudinal review of vascular findings in three individuals.Am J Med Genet A. 2020 May;182(5):1243-1248. doi: 10.1002/ajmg.a.61521. Epub 2020 Feb 17. Am J Med Genet A. 2020. PMID: 32065455
-
Cantù syndrome: Report of a patient with a novel variant in KCNJ8 and revision of literature.Am J Med Genet A. 2022 Jun;188(6):1661-1666. doi: 10.1002/ajmg.a.62710. Epub 2022 Mar 3. Am J Med Genet A. 2022. PMID: 35243770 Review.
-
Three patients with the osteochondrodysplasia and hypertrichosis syndrome--Cantu syndrome.Clin Dysmorphol. 1998 Apr;7(2):79-85. doi: 10.1097/00019605-199804000-00001. Clin Dysmorphol. 1998. PMID: 9571276 Review.
References
-
- Grange DK, Nichols CG, Singh GK, et al. Cantú syndrome. In: Adam MP, Everman DB, Mirzaa GM, et al., editors. GeneReviews. Seattle: University of Washington; 1993. - PubMed
-
- Lazalde B, Sanchez-Urbina R, Nuno-Arana I, Bitar WE, de Lourdes Ramirez-Duenas M. Autosomal dominant inheritance in Cantú syndrome (congenital hypertrichosis, osteochondrodysplasia, and cardiomegaly) Am J Med Genet. 2000;94(5):421–427. doi: 10.1002/1096-8628(20001023)94:5<421::AID-AJMG15>3.0.CO;2-9. - DOI - PubMed
-
- Brownstein CA, Towne MC, Luquette LJ, Harris DJ, Marinakis NS, Meinecke P, et al. Mutation of KCNJ8 in a patient with Cantú syndrome with unique vascular abnormalities – support for the role of K(atp) channels in this condition. Eur J Med Genet. 2013;56(12):678–682. doi: 10.1016/j.ejmg.2013.09.009. - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
