

Most Fractures Treated Nonoperatively in Individuals With Fibrodysplasia Ossificans Progressiva Heal With a Paucity of Flareups, Heterotopic Ossification, and Loss of Mobility
- PMID: 37156007
- PMCID: PMC10642855
- DOI: 10.1097/CORR.0000000000002672
Most Fractures Treated Nonoperatively in Individuals With Fibrodysplasia Ossificans Progressiva Heal With a Paucity of Flareups, Heterotopic Ossification, and Loss of Mobility
Abstract
Background: Fibrodysplasia ossificans progressiva (FOP) is an ultrarare genetic disorder with episodic and progressive heterotopic ossification. Tissue trauma is a major risk factor for flareups, heterotopic ossification (HO), and loss of mobility in patients with FOP. The International Clinical Council on FOP generally recommends avoiding surgery in patients with FOP unless the situation is life-threatening, because soft tissue injury can trigger an FOP flareup. Surprisingly little is known about flareups, HO formation, and loss of mobility after fractures of the normotopic (occurring in the normal place, distinct from heterotopic) skeleton when treated nonoperatively in patients with FOP.
Questions/purposes: (1) What proportion of fractures had radiographic evidence of union (defined as radiographic evidence of healing at 6 weeks) or nonunion (defined as the radiographic absence of a bridging callus at 3 years after the fracture)? (2) What proportion of patients had clinical symptoms of an FOP flareup because of the fracture (defined by increased pain or swelling at the fracture site within several days after closed immobilization)? (3) What proportion of patients with fractures had radiographic evidence of HO? (4) What proportion of patients lost movement after a fracture?
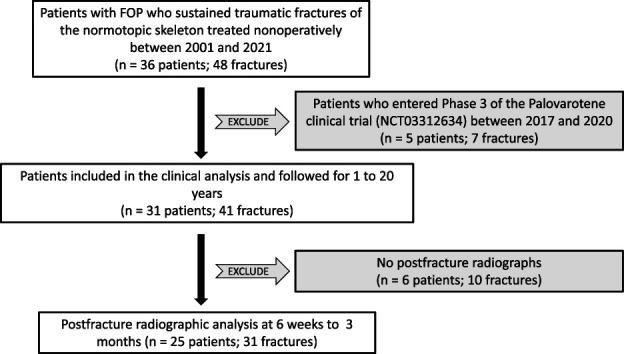
Methods: We retrospectively identified 36 patients with FOP from five continents who sustained 48 fractures of the normotopic skeleton from January 2001 to February 2021, who were treated nonoperatively, and who were followed for a minimum of 18 months after the fracture and for as long as 20 years, depending on when they sustained their fracture during the study period. Five patients (seven fractures) were excluded from the analysis to minimize cotreatment bias because these patients were enrolled in palovarotene clinical trials (NCT02190747 and NCT03312634) at the time of their fractures. Thus, we analyzed 31 patients (13 male, 18 female, median age 22 years, range 5 to 57 years) who sustained 41 fractures of the normotopic skeleton that were treated nonoperatively. Patients were analyzed at a median follow-up of 6 years (range 18 months to 20 years), and none was lost to follow-up. Clinical records for each patient were reviewed by the referring physician-author and the following data for each fracture were recorded: biological sex, ACVR1 gene pathogenic variant, age at the time of fracture, fracture mechanism, fracture location, initial treatment modality, prednisone use at the time of the fracture as indicated in the FOP Treatment Guidelines for flare prevention (2 mg/kg once daily for 4 days), patient-reported flareups (episodic inflammatory lesions of muscle and deep soft connective tissue characterized variably by swelling, escalating pain, stiffness, and immobility) after the fracture, follow-up radiographs of the fracture if available, HO formation (yes or no) as a result of the fracture determined at a minimum of 6 weeks after the fracture, and patient-reported loss of motion at least 6 months after and as long as 20 years after the fracture. Postfracture radiographs were available in 76% (31 of 41) of fractures in 25 patients and were independently reviewed by the referring physician-author and senior author for radiographic criteria of fracture healing and HO.
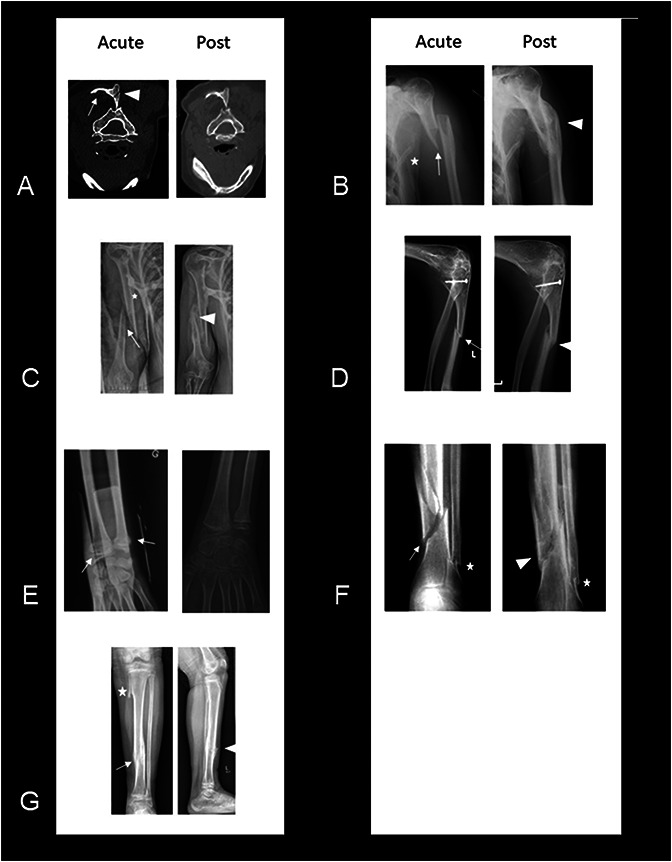
Results: Radiographic healing was noted in 97% (30 of 31) of fractures at 6 weeks after the incident fracture. Painless nonunion was noted in one patient who sustained a displaced patellar fracture and HO. In seven percent (three of 41) of fractures, patients reported increased pain or swelling at or near the fracture site within several days after fracture immobilization that likely indicated a site-specific FOP flareup. The same three patients reported a residual loss of motion 1 year after the fracture compared with their prefracture status. HO developed in 10% (three of 31) of the fractures for which follow-up radiographs were available. Patient-reported loss of motion occurred in 10% (four of 41) of fractures. Two of the four patients reported noticeable loss of motion and the other two patients reported that the joint was completely immobile (ankylosis).
Conclusion: Most fractures treated nonoperatively in individuals with FOP healed with few flareups, little or no HO, and preservation of mobility, suggesting an uncoupling of fracture repair and HO, which are two inflammation-induced processes of endochondral ossification. These findings underscore the importance of considering nonoperative treatment for fractures in individuals with FOP. Physicians who treat fractures in patients with FOP should consult with a member of the International Clinical Council listed in the FOP Treatment Guidelines ( https://www.iccfop.org ).
Level of evidence: Level IV, therapeutic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Figures

Similar articles
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Using Experience Sampling Methodology to Capture Disclosure Opportunities for Autistic Adults.Autism Adulthood. 2023 Dec 1;5(4):389-400. doi: 10.1089/aut.2022.0090. Epub 2023 Dec 12. Autism Adulthood. 2023. PMID: 38116059 Free PMC article.
-
Far Posterior Approach for Rib Fracture Fixation: Surgical Technique and Tips.JBJS Essent Surg Tech. 2024 Dec 6;14(4):e23.00094. doi: 10.2106/JBJS.ST.23.00094. eCollection 2024 Oct-Dec. JBJS Essent Surg Tech. 2024. PMID: 39650795 Free PMC article.
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
-
Trends in Surgical and Nonsurgical Aesthetic Procedures: A 14-Year Analysis of the International Society of Aesthetic Plastic Surgery-ISAPS.Aesthetic Plast Surg. 2024 Oct;48(20):4217-4227. doi: 10.1007/s00266-024-04260-2. Epub 2024 Aug 5. Aesthetic Plast Surg. 2024. PMID: 39103642 Review.
References
-
- Dijkman BG, Sprague S, Schemitsch EH, Bhandari M. When is a fracture healed? Radiographic and clinical criteria revisited. J Orthop Trauma. 2010;24:S76-S80. - PubMed
-
- Einhorn TA, Kaplan FS. Traumatic fractures of heterotopic bone in patients who have fibrodysplasia ossificans progressiva. Clin Orthop Relat Res.1994;308:173-177. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
