

Inhibition of C3 with pegcetacoplan results in normalization of hemolysis markers in paroxysmal nocturnal hemoglobinuria
- PMID: 35869170
- PMCID: PMC9375762
- DOI: 10.1007/s00277-022-04903-x
Inhibition of C3 with pegcetacoplan results in normalization of hemolysis markers in paroxysmal nocturnal hemoglobinuria
Abstract
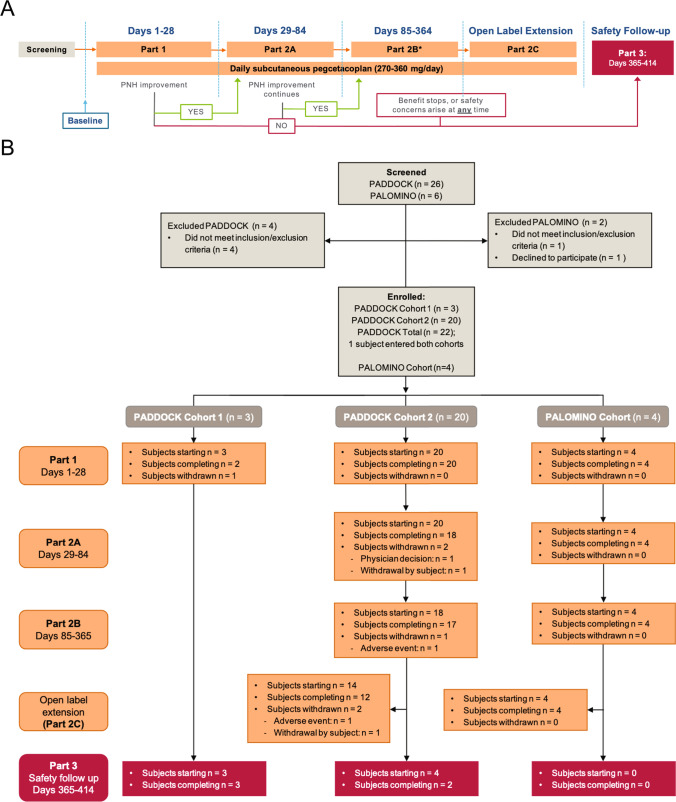
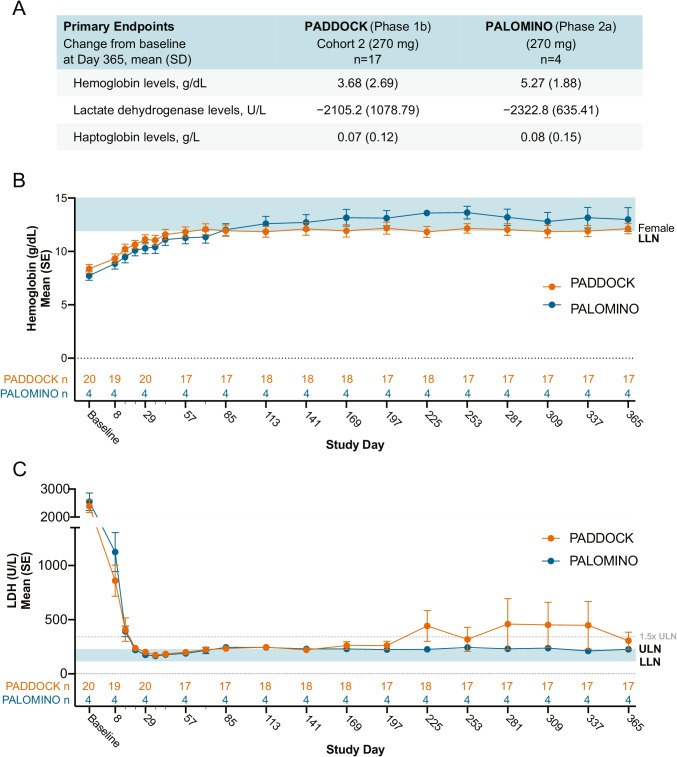
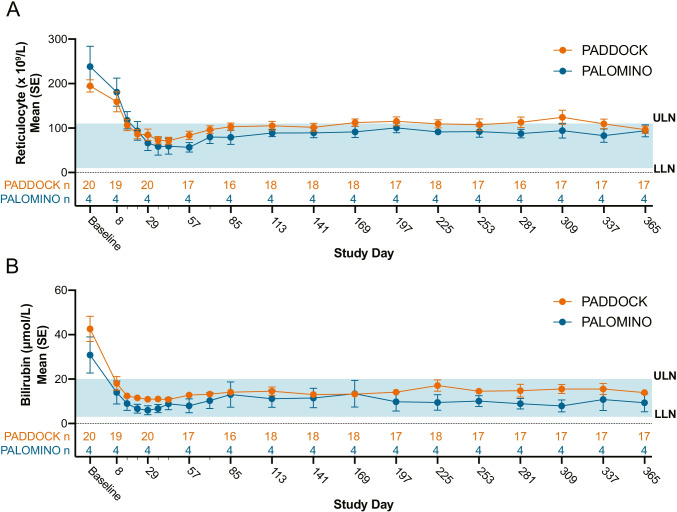
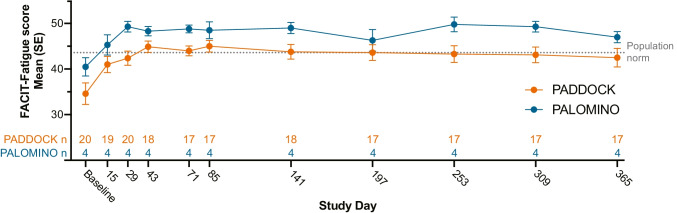
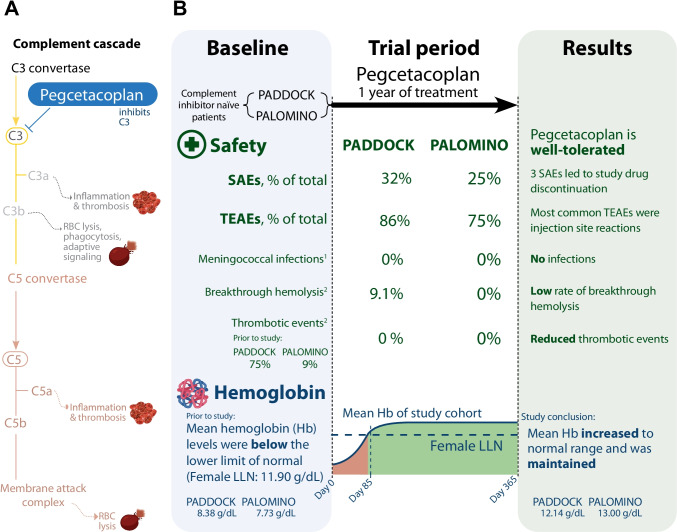
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, acquired hematologic disorder characterized by complement-mediated hemolysis. C5 inhibitors (eculizumab/ravulizumab) control intravascular hemolysis but do not prevent residual extravascular hemolysis. The newly approved complement inhibitor, pegcetacoplan, inhibits C3, upstream of C5, and has the potential to improve control of complement-mediated hemolysis. The PADDOCK and PALOMINO clinical trials assessed the safety and efficacy of pegcetacoplan in complement inhibitor-naïve adults (≥ 18 years) diagnosed with PNH. Patients in PADDOCK (phase 1b open-label, pilot trial) received daily subcutaneous pegcetacoplan (cohort 1: 180 mg up to day 28 [n = 3]; cohort 2: 270-360 mg up to day 365 [n = 20]). PALOMINO (phase 2a, open-label trial) used the same dosing protocol as PADDOCK cohort 2 (n = 4). Primary endpoints in both trials were mean change from baseline in hemoglobin, lactate dehydrogenase, haptoglobin, and the number and severity of treatment-emergent adverse events. Mean baseline hemoglobin levels were below the lower limit of normal in both trials (PADDOCK: 8.38 g/dL; PALOMINO: 7.73 g/dL; normal range: 11.90-18.00 g/dL), increased to within normal range by day 85, and were sustained through day 365 (PADDOCK: 12.14 g/dL; PALOMINO: 13.00 g/dL). In PADDOCK, 3 serious adverse events (SAE) led to study drug discontinuation, 1 of which was deemed likely related to pegcetacoplan and 1 SAE, not deemed related to study drug, led to death. No SAE led to discontinuation/death in PALOMINO. Pegcetacoplan was generally well tolerated and improved hematological parameters by controlling hemolysis, while also improving other clinical PNH indicators in both trials. These trials were registered at www.clinicaltrials.gov (NCT02588833 and NCT03593200).
Keywords: Hemoglobin; LDH; Paroxysmal nocturnal hemoglobinuria (PNH); Phase I/II trials; Quality of life; Safety.
© 2022. The Author(s).
Conflict of interest statement
Raymond S. M. Wong: Alexion: consultancy, honoraria, research funding, and speakers bureau; Apellis: research funding and speakers bureau; Roche: consultancy, honoraria, research funding, and speakers bureau
Humphrey W. H. Pullon: none
Ismail Amine: is a full-time employee of Acibadem City Clinic Tokuda Hospital.
Andrija Bogdanovic: Novartis: consultancy, membership on an entity’s board of directors or advisory committees, and speaker’s bureau; Takeda: membership on an entity’s board of directors or advisory committees, and speaker’s bureau; Pfizer: membership on an entity’s board of directors or advisory committees; Apellis: investigator fee in clinical trial
Pascal Deschatelets is an inventor on patents (planned, issued, or pending) and is the founder and CSO of Apellis Pharmaceuticals.
Cedric G. Francois is an inventor on patents (planned, issued, or pending) and the founder and CEO of Apellis Pharmaceuticals.
Kalina Ignatova: None
Surapol Issaragrisil: Alexion: speakers bureau; Novartis: speakers bureau
Pimjai Niparuck: none
Tontanai Numbenjapon: none
Eloy Roman: Alexion: speakers bureau; Novartis: speakers bureau
Jameela Sathar: Roche: honoraria; Novo Nordisk: honoraria; Bayer: honoraria
Raymond Xu is a full-time employee of Apellis Pharmaceuticals.
Mohammed Al-Adhami is a full-time employee of Apellis Pharmaceuticals.
Lisa Tan as a consultant and is an inventor on patents (planned, issued, or pending) for Apellis Pharmaceuticals.
Eric Tse: MSD: research funding; Janssen: research funding
Federico V. Grossi is an inventor on patents (planned, issued, or pending) and is the CMO of Apellis Pharmaceuticals.
Figures
Similar articles
-
Pegcetacoplan versus Eculizumab in Paroxysmal Nocturnal Hemoglobinuria.N Engl J Med. 2021 Mar 18;384(11):1028-1037. doi: 10.1056/NEJMoa2029073. N Engl J Med. 2021. PMID: 33730455 Clinical Trial.
-
Improvements in hematologic markers and decreases in fatigue with pegcetacoplan for patients with paroxysmal nocturnal hemoglobinuria and mild or moderate anemia (hemoglobin ≥10 g/dL) who had received eculizumab or were naive to complement inhibitors.PLoS One. 2024 Jul 29;19(7):e0306407. doi: 10.1371/journal.pone.0306407. eCollection 2024. PLoS One. 2024. PMID: 39079163 Free PMC article. Clinical Trial.
-
Pegcetacoplan: A Review in Paroxysmal Nocturnal Haemoglobinuria.Drugs. 2022 Dec;82(18):1727-1735. doi: 10.1007/s40265-022-01809-w. Epub 2022 Dec 2. Drugs. 2022. PMID: 36459381 Free PMC article. Review.
-
Safety and efficacy of pegcetacoplan in paroxysmal nocturnal hemoglobinuria.Ther Adv Hematol. 2022 Jul 28;13:20406207221114673. doi: 10.1177/20406207221114673. eCollection 2022. Ther Adv Hematol. 2022. PMID: 35923770 Free PMC article. Review.
-
Pegcetacoplan controls hemolysis in complement inhibitor-naive patients with paroxysmal nocturnal hemoglobinuria.Blood Adv. 2023 Jun 13;7(11):2468-2478. doi: 10.1182/bloodadvances.2022009129. Blood Adv. 2023. PMID: 36848639 Free PMC article. Clinical Trial.
Cited by
-
Moving toward Individual Treatment Goals with Pegcetacoplan in Patients with PNH and Impaired Bone Marrow Function.Int J Mol Sci. 2024 Aug 6;25(16):8591. doi: 10.3390/ijms25168591. Int J Mol Sci. 2024. PMID: 39201278 Free PMC article. Clinical Trial.
-
Thrombosis and meningococcal infection rates in pegcetacoplan-treated patients with paroxysmal nocturnal hemoglobinuria in the clinical trial and postmarketing settings.Res Pract Thromb Haemost. 2024 Apr 24;8(4):102416. doi: 10.1016/j.rpth.2024.102416. eCollection 2024 May. Res Pract Thromb Haemost. 2024. PMID: 38812989 Free PMC article.
-
Navigating the Complement Pathway to Optimize PNH Treatment with Pegcetacoplan and Other Currently Approved Complement Inhibitors.Int J Mol Sci. 2024 Aug 31;25(17):9477. doi: 10.3390/ijms25179477. Int J Mol Sci. 2024. PMID: 39273426 Free PMC article. Review.
-
Paroxysmal Nocturnal Hemoglobinuria: Biology and Treatment.Medicina (Kaunas). 2023 Sep 6;59(9):1612. doi: 10.3390/medicina59091612. Medicina (Kaunas). 2023. PMID: 37763731 Free PMC article. Review.
-
Safety and Efficacy of Pegcetacoplan in Adult Patients with Paroxysmal Nocturnal Hemoglobinuria over 48 Weeks: 307 Open-Label Extension Study.Adv Ther. 2024 May;41(5):2050-2069. doi: 10.1007/s12325-024-02827-8. Epub 2024 Apr 4. Adv Ther. 2024. PMID: 38573482 Free PMC article.
References
-
- Risitano AM, Notaro R, Marando L, Serio B, Ranaldi D, Seneca E, Ricci P, Alfinito F, Camera A, Gianfaldoni G, Amendola A, Boschetti C, Di Bona E, Fratellanza G, Barbano F, Rodeghiero F, Zanella A, Iori AP, Selleri C, Luzzatto L, Rotoli B. Complement fraction 3 binding on erythrocytes as additional mechanism of disease in paroxysmal nocturnal hemoglobinuria patients treated by eculizumab. Blood. 2009;113(17):4094–4100. doi: 10.1182/blood-2008-11-189944. - DOI - PubMed
-
- Ullman AS, Horn RCJ, Abraham JP, VanSlyck EJ. Paroxysmal nocturnal hemoglobinuria: report of two cases with atypical features, autopsy findings, and review of pathophysiology. Henry Ford Hosp Med Bull. 1963;11(2):135–145. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
