

Natural History of Obesity Due to POMC, PCSK1, and LEPR Deficiency and the Impact of Setmelanotide
- PMID: 35528826
- PMCID: PMC9070354
- DOI: 10.1210/jendso/bvac057
Natural History of Obesity Due to POMC, PCSK1, and LEPR Deficiency and the Impact of Setmelanotide
Abstract
Context: Rare homozygous or biallelic variants in POMC, PCSK1, and LEPR can disrupt signaling through the melanocortin-4 receptor (MC4R) pathway, resulting in hyperphagia and severe early-onset obesity. In pivotal Phase 3 clinical trials, treatment with the MC4R agonist setmelanotide reduced hunger and weight in patients with obesity due to proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency.
Objective: To characterize the historical weight trajectory in these patients.
Methods: This analysis included data from 2 pivotal single-arm, open-label, Phase 3 trials (NCT02896192, NCT03287960). These were multicenter trials. Patients had obesity due to POMC/PCSK1 or LEPR deficiency. During the trial, patients were treated with setmelanotide. Historical data on measured weight and height were obtained during screening.
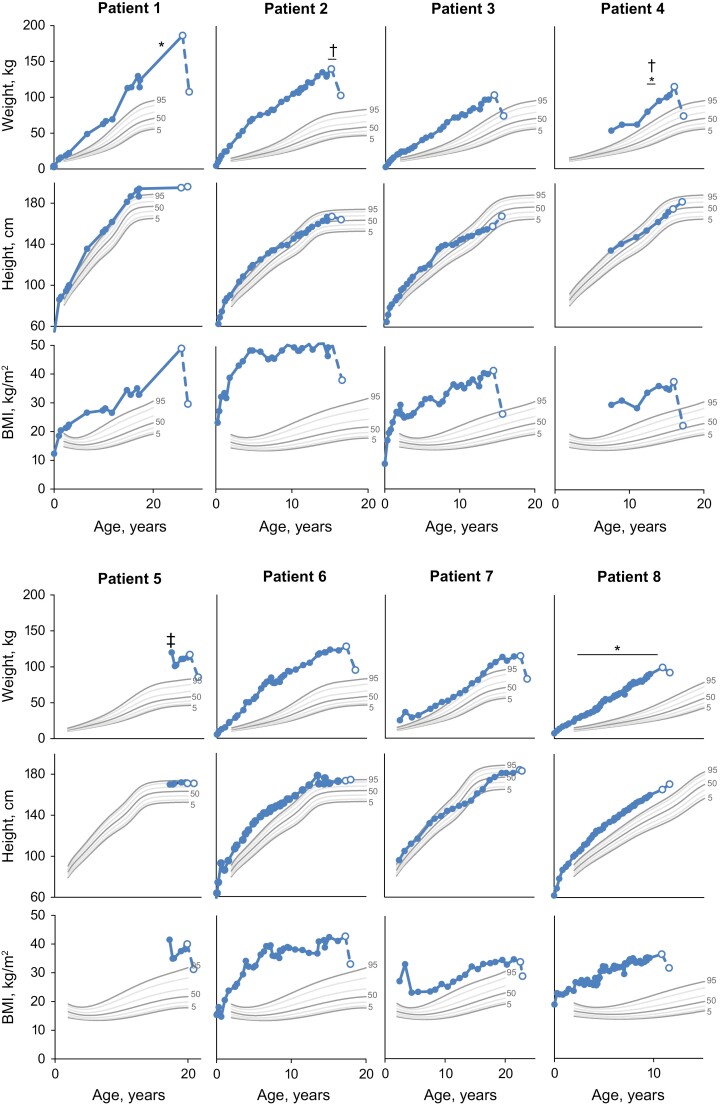
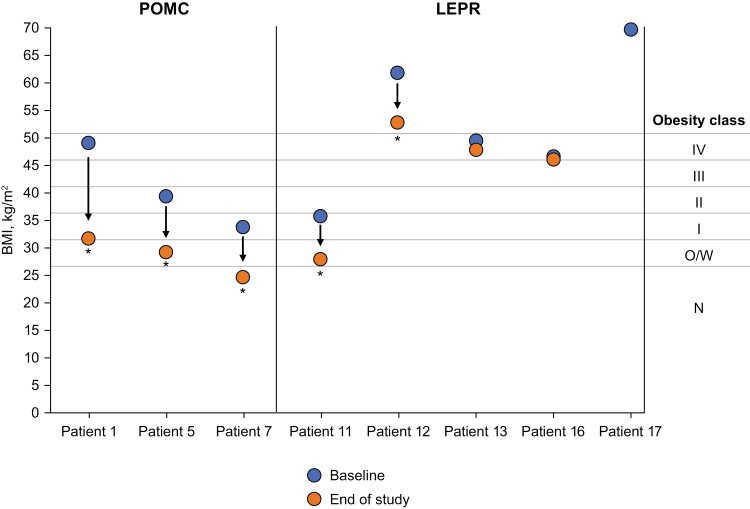
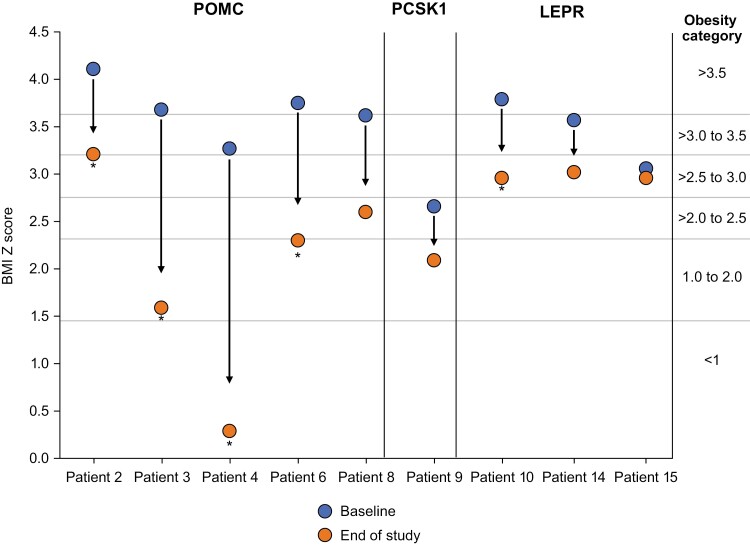
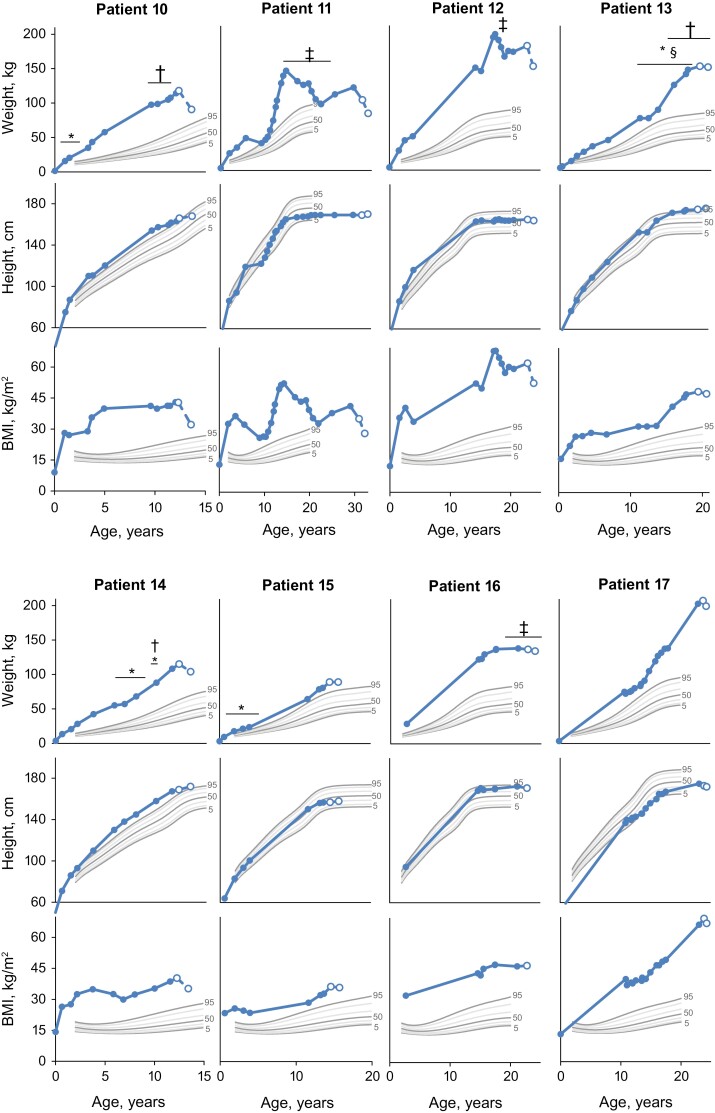
Results: A total of 17 patients (POMC, n = 8; PCSK1, n = 1; LEPR, n = 8) with historical weight and height data were included in this analysis. Before setmelanotide treatment, patients with obesity due to POMC/PCSK1 or LEPR deficiency were above the 95th percentile for weight throughout childhood, demonstrated continuous weight gain, and did not show long-term weight loss upon interventions (eg, diet, surgery, exercise). Setmelanotide treatment attenuated weight and body mass index trajectories over the observation period of 1 year.
Conclusion: In patients with POMC, PCSK1, or LEPR deficiency, traditional interventions for weight loss had limited impact on the trajectory of severe early-onset obesity. However, setmelanotide treatment attenuated weight and body mass index trajectories and led to weight loss associated with health benefits in most individuals.
Keywords: LEPR; MC4R pathway; POMC; obesity; setmelanotide.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: single-arm, open-label, multicentre, phase 3 trials.Lancet Diabetes Endocrinol. 2020 Dec;8(12):960-970. doi: 10.1016/S2213-8587(20)30364-8. Epub 2020 Oct 30. Lancet Diabetes Endocrinol. 2020. PMID: 33137293 Clinical Trial.
-
Setmelanotide: a promising advancement for pediatric patients with rare forms of genetic obesity.Curr Opin Endocrinol Diabetes Obes. 2023 Apr 1;30(2):136-140. doi: 10.1097/MED.0000000000000798. Epub 2023 Feb 1. Curr Opin Endocrinol Diabetes Obes. 2023. PMID: 36722447 Free PMC article. Review.
-
Setmelanotide: First Approval.Drugs. 2021 Feb;81(3):397-403. doi: 10.1007/s40265-021-01470-9. Drugs. 2021. PMID: 33638809 Review.
-
Beneficial Effects of Setmelanotide in a 5-Year-Old Boy With POMC Deficiency and on His Caregivers.JCEM Case Rep. 2023 Jun 15;1(3):luad041. doi: 10.1210/jcemcr/luad041. eCollection 2023 May. JCEM Case Rep. 2023. PMID: 37908575 Free PMC article.
-
Melanocortin 4 Receptor Pathway Dysfunction in Obesity: Patient Stratification Aimed at MC4R Agonist Treatment.J Clin Endocrinol Metab. 2018 Jul 1;103(7):2601-2612. doi: 10.1210/jc.2018-00258. J Clin Endocrinol Metab. 2018. PMID: 29726959 Free PMC article.
Cited by
-
[Improved Care and Treatment Options for Patients with Hyperphagia-Associated Obesity in Bardet-Biedl Syndrome].Klin Padiatr. 2024 Sep;236(5):269-279. doi: 10.1055/a-2251-5382. Epub 2024 Mar 8. Klin Padiatr. 2024. PMID: 38458231 Free PMC article. Review. German.
-
Naringenin and β-carotene convert human white adipocytes to a beige phenotype and elevate hormone- stimulated lipolysis.Front Endocrinol (Lausanne). 2023 Apr 17;14:1148954. doi: 10.3389/fendo.2023.1148954. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37143734 Free PMC article.
-
Setmelanotide: A Melanocortin-4 Receptor Agonist for the Treatment of Severe Obesity Due to Hypothalamic Dysfunction.touchREV Endocrinol. 2024 Oct;20(2):62-71. doi: 10.17925/EE.2024.20.2.9. Epub 2024 Feb 9. touchREV Endocrinol. 2024. PMID: 39526054 Free PMC article. Review.
-
Special considerations for the child with obesity: An Obesity Medicine Association (OMA) clinical practice statement (CPS) 2024.Obes Pillars. 2024 May 23;11:100113. doi: 10.1016/j.obpill.2024.100113. eCollection 2024 Sep. Obes Pillars. 2024. PMID: 38953014 Free PMC article.
-
Current and future state of pharmacological management of pediatric obesity.Int J Obes (Lond). 2024 Feb 6. doi: 10.1038/s41366-024-01465-y. Online ahead of print. Int J Obes (Lond). 2024. PMID: 38321079 Review.
References
-
- van der Klaauw AA, Farooqi IS. The hunger genes: pathways to obesity. Cell. 2015;161(1):119-132. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous