

Population pharmacokinetic modeling and simulations of berotralstat for prophylactic treatment of attacks of hereditary angioedema
- PMID: 35212456
- PMCID: PMC9010267
- DOI: 10.1111/cts.13233
Population pharmacokinetic modeling and simulations of berotralstat for prophylactic treatment of attacks of hereditary angioedema
Abstract
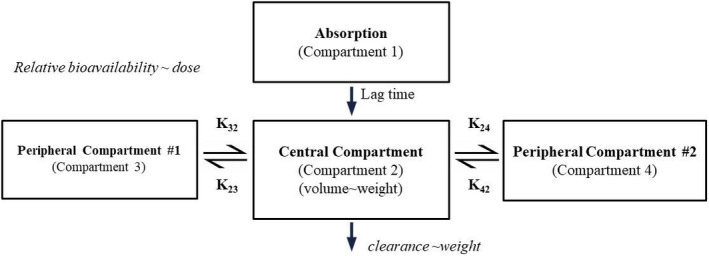
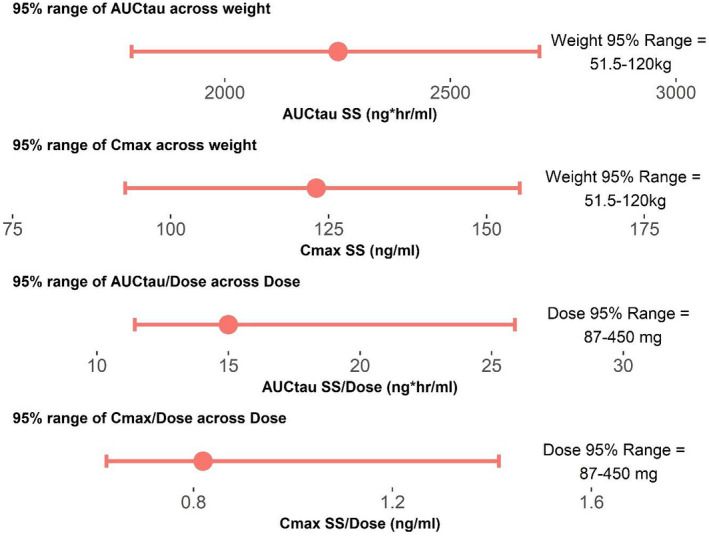
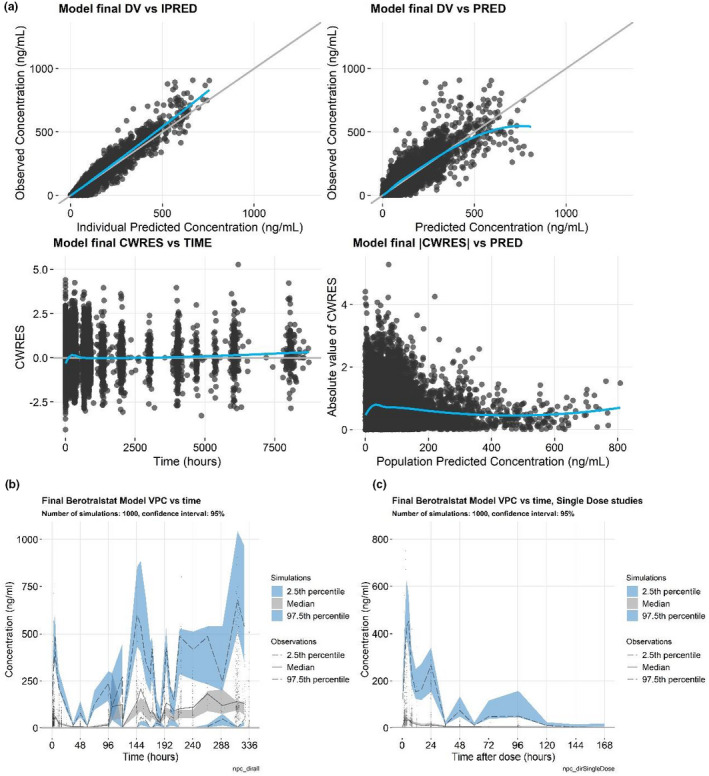
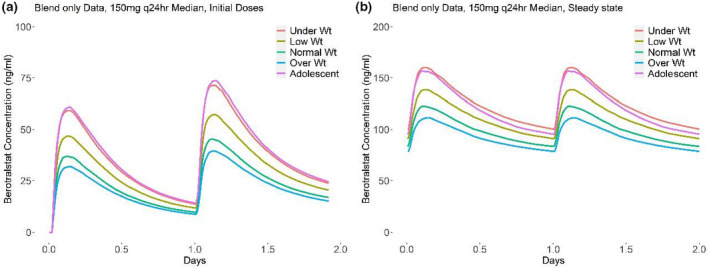
Hereditary angioedema (HAE) is an autosomal dominant disorder characterized by recurrent episodes of swelling of the skin, larynx, gastrointestinal tract, genitals, and extremities that can be disruptive to patient quality of life. Dysregulation of plasma kallikrein activity leads to increased production and accumulation of bradykinin in HAE and causes attacks of angioedema. Plasma kallikrein is a serine protease essential for the formation of bradykinin. Berotralstat is a potent, highly selective, orally bioavailable small-molecule plasma kallikrein inhibitor that has been approved to prevent attacks of HAE in adults and children 12 years of age and older. Population pharmacokinetic (PK) analyses were conducted to describe the PK of berotralstat (BCX7353; Orladeyo™ ) and to evaluate the covariates that may explain variability in PK. The PK of berotralstat were characterized by population PK modeling of data from 13 clinical studies and a total of 771 healthy subjects and patients with HAE. The PK profile was well described by a three-compartment model with first-order absorption including an absorption lag time and linear elimination. Among the covariates tested, the effects of bilirubin and food were found not to be clinically significant and were removed from the model. Covariate analysis indicated significant effects of dose on bioavailability and weight on berotralstat clearance and volume. Despite the covariate effect of weight, simulations in adolescents and adults who were underweight, low weight, and overweight demonstrated similar predicted exposures to those observed at therapeutic doses in a clinical trial. Therefore, no dose adjustment is required in these HAE patient subpopulations.
© 2022 BioCryst Pharmaceuticals, Inc. Clinical and Translational Science published by Wiley Periodicals LLC on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
M.C. and W.P.S. are current employees at BioCryst Pharmaceuticals, Inc. A.M. and S.M. were previously employed by BioCryst Pharmaceuticals, Inc. M.S. is a compensated consultant to BioCryst Pharmaceuticals, Inc.
Figures
Similar articles
-
[Pharmacological and clinical study results of Berotralstat Hydrochloride for long-term prophylactic treatment of hereditary angioedema].Nihon Yakurigaku Zasshi. 2021;156(6):382-390. doi: 10.1254/fpj.21069. Nihon Yakurigaku Zasshi. 2021. PMID: 34719573 Japanese.
-
Berotralstat: First Approval.Drugs. 2021 Feb;81(3):405-409. doi: 10.1007/s40265-021-01475-4. Drugs. 2021. PMID: 33646555 Review.
-
Berotralstat (BCX7353) is a novel oral prophylactic treatment for hereditary angioedema: Review of phase II and III studies.Allergy Asthma Proc. 2021 Jul 14;42(4):274-282. doi: 10.2500/aap.2021.42.210034. Epub 2021 Jun 14. Allergy Asthma Proc. 2021. PMID: 34127176 Review.
-
Oral once-daily berotralstat for the prevention of hereditary angioedema attacks: A randomized, double-blind, placebo-controlled phase 3 trial.J Allergy Clin Immunol. 2021 Jul;148(1):164-172.e9. doi: 10.1016/j.jaci.2020.10.015. Epub 2020 Oct 21. J Allergy Clin Immunol. 2021. PMID: 33098856 Clinical Trial.
-
Discovery and optimization of orally bioavailable and potent plasma Kallikrein inhibitors bearing a quaternary carbon.Bioorg Med Chem. 2022 Nov 1;73:117035. doi: 10.1016/j.bmc.2022.117035. Epub 2022 Sep 30. Bioorg Med Chem. 2022. PMID: 36208543
Cited by
-
Doses Evaluated in Clinical Pharmacology Studies Investigating the Effect of Intrinsic and Extrinsic Factors on PK and Safety: Case Examples from Approved Drug Development Programs.AAPS J. 2024 Jun 17;26(4):71. doi: 10.1208/s12248-024-00935-5. AAPS J. 2024. PMID: 38886275 Review.
-
Consensus on diagnosis and management of Hereditary Angioedema in the Middle East: A Delphi initiative.World Allergy Organ J. 2022 Dec 24;16(1):100729. doi: 10.1016/j.waojou.2022.100729. eCollection 2023 Jan. World Allergy Organ J. 2022. PMID: 36601261 Free PMC article.
-
Pyrazole-containing pharmaceuticals: target, pharmacological activity, and their SAR studies.RSC Med Chem. 2022 Aug 26;13(11):1300-1321. doi: 10.1039/d2md00206j. eCollection 2022 Nov 16. RSC Med Chem. 2022. PMID: 36439976 Free PMC article. Review.
References
-
- Longhurst H, Cicardi M. Hereditary angio‐oedema. Lancet. 2012;379:474‐481. - PubMed
-
- Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA medical advisory board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract. 2021;9:132‐150 e133. - PubMed
-
- Maurer M, Magerl M, Ansotegui I, et al. The international WAO/EAACI guideline for the management of hereditary angioedema‐The 2017 revision and update. Allergy. 2018;73:1575‐1596. - PubMed
-
- Kaplan AP, Joseph K. The bradykinin‐forming cascade and its role in hereditary angioedema. Ann Allergy Asthma Immunol. 2010;104:193‐204. - PubMed
-
- Zuraw BL, Christiansen SC. HAE pathophysiology and underlying mechanisms. Clin Rev Allergy Immunol. 2016;51:216‐229. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
