Improving the quality of nursing documentation at a residential care home: a clinical audit
- PMID: 34154606
- PMCID: PMC8215798
- DOI: 10.1186/s12912-021-00629-9
Improving the quality of nursing documentation at a residential care home: a clinical audit
Abstract
Background: Quality in nursing documentation holds promise to increase patient safety and quality of care. While high-quality nursing documentation implies a comprehensive documentation of the nursing process, nursing records do not always adhere to these documentation criteria. The aim of this quality improvement project was to assess the quality of electronic nursing records in a residential care home using a standardized audit tool and, if necessary, implement a tailored strategy to improve documentation practice.
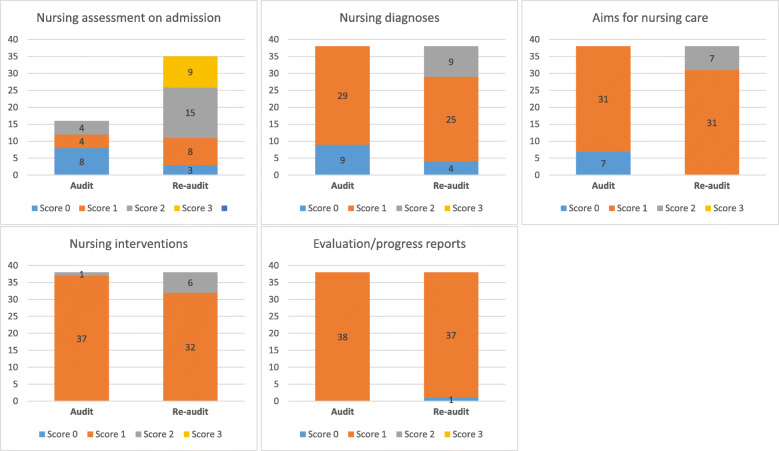
Methods: A criteria-based clinical audit was performed in a residential care home in Norway. Quantitative criteria in the N-Catch II audit instrument was used to give an assessment of electronic nursing records on the following: nursing assessment on admission, nursing diagnoses, aims for nursing care, nursing interventions, and evaluation/progress reports. Each criterium was scored on a 0-3 point scale, with standard (complete documentation) coinciding with the highest score. A retrospective audit was conducted on 38 patient records from January to March 2018, followed by the development and execution of an implementation strategy tailored to local barriers. A re-audit was performed on 38 patient records from March to June 2019.
Results: None of the investigated patient records at audit fulfilled standards for recommended nursing documentation practice. Mean scores at audit varied from 0.4 (95 % confidence interval 0.3-0.6) for "aims for nursing care" to 1.1 (0.9-1.3) for "nursing diagnoses". After implementation of a tailored multifaceted intervention strategy, an improvement (p < 0.001) was noted for all criteria except for "evaluation/progress reports" (p = 0.6). The improvement did not lead to standards being met at re-audit, where mean scores varied from 0.9 (0.8-1.1) for "evaluation/progress reports" to 1.9 (1.5-2.2) for "nursing assessment on admission".
Conclusions: A criteria-based clinical audit with multifaceted tailored interventions that addresses determinants of practice may improve the quality of nursing documentation, but further cycles of the clinical audit process are needed before standards are met and focus can be shifted to sustainment of knowledge use.
Keywords: Nursing; audit; electronic health records; nursing records.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Assessment of quality in psychiatric nursing documentation - a clinical audit.BMC Nurs. 2014 Oct 17;13:32. doi: 10.1186/1472-6955-13-32. eCollection 2014. BMC Nurs. 2014. PMID: 25349532 Free PMC article.
-
The quality of paper-based versus electronic nursing care plan in Australian aged care homes: A documentation audit study.Int J Med Inform. 2015 Aug;84(8):561-9. doi: 10.1016/j.ijmedinf.2015.04.004. Epub 2015 May 8. Int J Med Inform. 2015. PMID: 26004340
-
Quality of nursing documentation: Paper-based health records versus electronic-based health records.J Clin Nurs. 2018 Feb;27(3-4):e578-e589. doi: 10.1111/jocn.14097. Epub 2017 Nov 20. J Clin Nurs. 2018. PMID: 28981172
-
Quality of nursing documentation and approaches to its evaluation: a mixed-method systematic review.J Adv Nurs. 2011 Sep;67(9):1858-75. doi: 10.1111/j.1365-2648.2011.05634.x. Epub 2011 Apr 6. J Adv Nurs. 2011. PMID: 21466578 Review.
-
A complex intervention to reduce avoidable hospital admissions in nursing homes: a research programme including the BHiRCH-NH pilot cluster RCT.Southampton (UK): NIHR Journals Library; 2021 Feb. Southampton (UK): NIHR Journals Library; 2021 Feb. PMID: 33651525 Free Books & Documents. Review.
Cited by
-
CONTACT: a non-randomised feasibility study of bluetooth-enabled wearables for contact tracing in UK care homes during the COVID-19 pandemic.Pilot Feasibility Stud. 2024 Oct 2;10(1):125. doi: 10.1186/s40814-024-01549-6. Pilot Feasibility Stud. 2024. PMID: 39358817 Free PMC article.
-
Guide for Systematization of Care and Nursing Process: educational technology for professional practice.Rev Bras Enferm. 2023 Apr 14;76Suppl 4(Suppl 4):e20210975. doi: 10.1590/0034-7167-2021-0975. eCollection 2023. Rev Bras Enferm. 2023. PMID: 37075359 Free PMC article. Review.
-
'Smart' BLE wearables for digital contact tracing in care homes during the COVID-19 pandemic-a process evaluation of the CONTACT feasibility study.Implement Sci Commun. 2023 Dec 4;4(1):155. doi: 10.1186/s43058-023-00533-0. Implement Sci Commun. 2023. PMID: 38049924 Free PMC article.
-
Improving Nursing Assessment in Adult Hospitalization Units: A Secondary Analysis.Nurs Rep. 2023 Aug 23;13(3):1148-1159. doi: 10.3390/nursrep13030099. Nurs Rep. 2023. PMID: 37755342 Free PMC article.
-
Documenting fall episodes: a scoping review.Front Public Health. 2023 May 2;11:1067243. doi: 10.3389/fpubh.2023.1067243. eCollection 2023. Front Public Health. 2023. PMID: 37200991 Free PMC article.
References
-
- Urquhart C, Currell R, Grant MJ, Hardiker NR. Nursing record systems: effects on nursing practice and healthcare outcomes. Cochrane Database Syst Reviews. 2009; (1). Available from: 10.1002/14651858.CD002099.pub2. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous