

Age-dependence of healthcare interventions for COVID-19 in Ontario, Canada
- PMID: 33845807
- PMCID: PMC8040357
- DOI: 10.1186/s12889-021-10611-4
Age-dependence of healthcare interventions for COVID-19 in Ontario, Canada
Abstract
Background: Patient age is one of the most salient clinical indicators of risk from COVID-19. Age-specific distributions of known SARS-CoV-2 infections and COVID-19-related deaths are available for many regions. Less attention has been given to the age distributions of serious medical interventions administered to COVID-19 patients, which could reveal sources of potential pressure on the healthcare system should SARS-CoV-2 prevalence increase, and could inform mass vaccination strategies. The aim of this study is to quantify the relationship between COVID-19 patient age and serious outcomes of the disease, beyond fatalities alone.
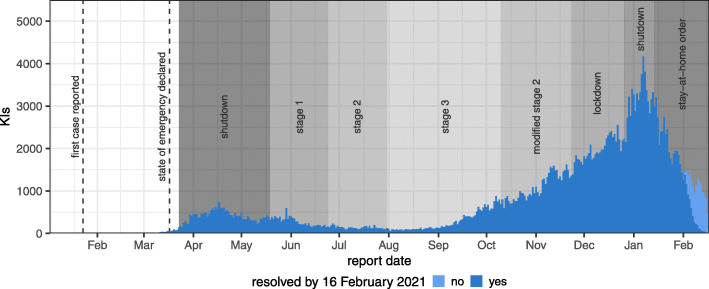
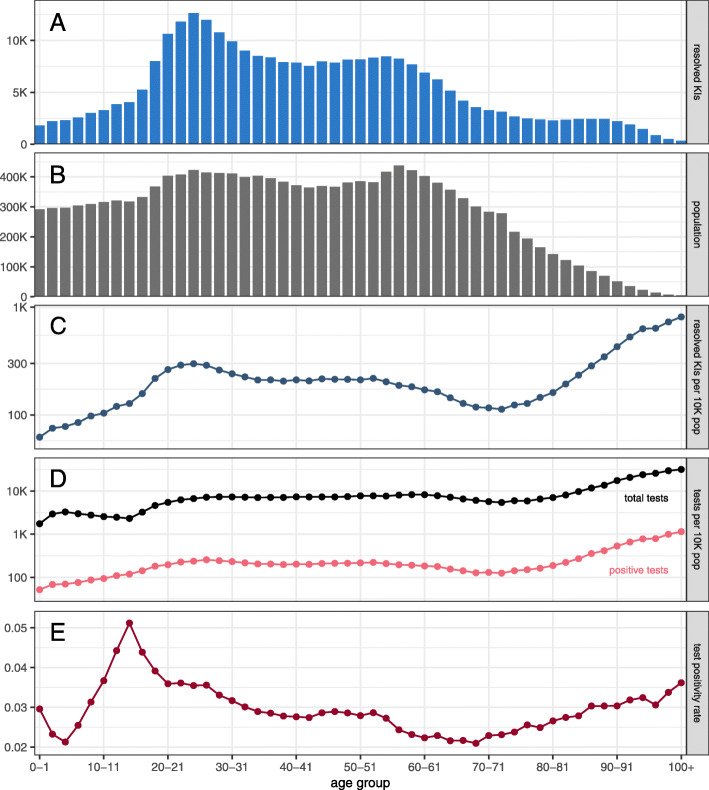
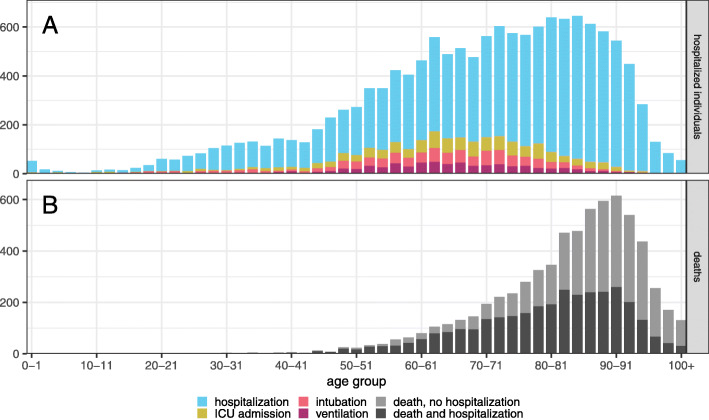
Methods: We analysed 277,555 known SARS-CoV-2 infection records for Ontario, Canada, from 23 January 2020 to 16 February 2021 and estimated the age distributions of hospitalizations, Intensive Care Unit admissions, intubations, and ventilations. We quantified the probability of hospitalization given known SARS-CoV-2 infection, and of survival given COVID-19-related hospitalization.
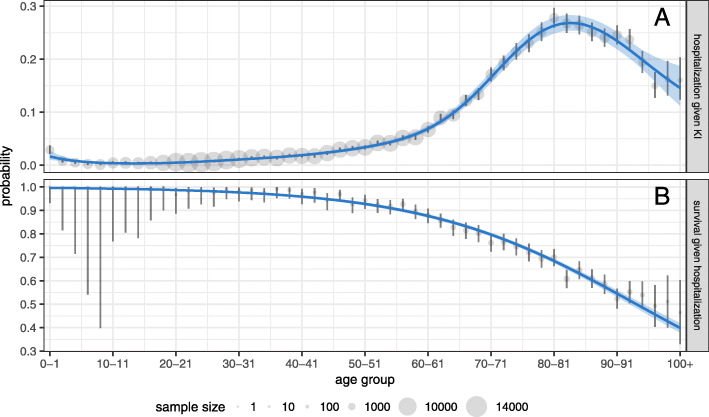
Results: The distribution of hospitalizations peaks with a wide plateau covering ages 60-90, whereas deaths are concentrated in ages 80+. The estimated probability of hospitalization given known infection reaches a maximum of 27.8% at age 80 (95% CI 26.0%-29.7%). The probability of survival given hospitalization is nearly 100% for adults younger than 40, but declines substantially after this age; for example, a hospitalized 54-year-old patient has a 91.7% chance of surviving COVID-19 (95% CI 88.3%-94.4%).
Conclusions: Our study demonstrates a significant need for hospitalization in middle-aged individuals and young seniors. This need is not captured by the distribution of deaths, which is heavily concentrated in very old ages. The probability of survival given hospitalization for COVID-19 is lower than is generally perceived for patients over 40. If acute care capacity is exceeded due to an increase in COVID-19 prevalence, the distribution of deaths could expand toward younger ages. These results suggest that vaccine programs should aim to prevent infection not only in old seniors, but also in young seniors and middle-aged individuals, to protect them from serious illness and to limit stress on the healthcare system.
Keywords: Age distribution; COVID-19; Epidemiology; Hospitalization; Infectious disease; SARS-CoV-2.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
SARS-CoV-2 Infection, Hospitalization, and Mortality in Adults With and Without Cancer.JAMA Netw Open. 2023 Aug 1;6(8):e2331617. doi: 10.1001/jamanetworkopen.2023.31617. JAMA Netw Open. 2023. PMID: 37651139 Free PMC article.
-
The impact of shifting demographics, variants of concern and vaccination on outcomes during the first 3 COVID-19 waves in Alberta and Ontario: a retrospective cohort study.CMAJ Open. 2022 Apr 26;10(2):E400-E408. doi: 10.9778/cmajo.20210323. Print 2022 Apr-Jun. CMAJ Open. 2022. PMID: 35473827 Free PMC article.
-
Vaccine effectiveness against hospitalization among adolescent and pediatric SARS-CoV-2 cases between May 2021 and January 2022 in Ontario, Canada: A retrospective cohort study.PLoS One. 2023 Mar 31;18(3):e0283715. doi: 10.1371/journal.pone.0283715. eCollection 2023. PLoS One. 2023. PMID: 37000810 Free PMC article.
-
Vaccination and non-pharmaceutical interventions for COVID-19: a mathematical modelling study.Lancet Infect Dis. 2021 Jun;21(6):793-802. doi: 10.1016/S1473-3099(21)00143-2. Epub 2021 Mar 18. Lancet Infect Dis. 2021. PMID: 33743847 Free PMC article.
-
Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance - One Hospital, California, July 15-September 23, 2021, and December 21, 2021-January 27, 2022.MMWR Morb Mortal Wkly Rep. 2022 Feb 11;71(6):217-223. doi: 10.15585/mmwr.mm7106e2. MMWR Morb Mortal Wkly Rep. 2022. PMID: 35143466 Free PMC article.
Cited by
-
Comparative assessment of methods for short-term forecasts of COVID-19 hospital admissions in England at the local level.BMC Med. 2022 Feb 21;20(1):86. doi: 10.1186/s12916-022-02271-x. BMC Med. 2022. PMID: 35184736 Free PMC article.
-
Weighted gene co-expression network analysis revealed T cell differentiation associated with the age-related phenotypes in COVID-19 patients.BMC Med Genomics. 2023 Mar 25;16(1):59. doi: 10.1186/s12920-023-01490-2. BMC Med Genomics. 2023. PMID: 36966292 Free PMC article.
-
Modelling the impact of age-stratified public health measures on SARS-CoV-2 transmission in Canada.R Soc Open Sci. 2021 Nov 2;8(11):210834. doi: 10.1098/rsos.210834. eCollection 2021 Nov. R Soc Open Sci. 2021. PMID: 34737875 Free PMC article.
-
Biochemistry tests in hospitalized COVID-19 patients: Experience from a Canadian tertiary care centre.Clin Biochem. 2021 Sep;95:41-48. doi: 10.1016/j.clinbiochem.2021.05.008. Epub 2021 May 19. Clin Biochem. 2021. PMID: 34022172 Free PMC article.
-
SARS-CoV-2 is associated with changes in brain structure in UK Biobank.Nature. 2022 Apr;604(7907):697-707. doi: 10.1038/s41586-022-04569-5. Epub 2022 Mar 7. Nature. 2022. PMID: 35255491 Free PMC article.
References
-
- Novel Coronavirus (2019-nCoV) Situation Report—1. World Health Organization. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 31 Jul 2020.
-
- WHO Coronavirus Disease (COVID-19) Dashboard. World Health Organization. 2021. https://covid19.who.int/table. Accessed 23 Feb 2021.
-
- Emerging COVID-19 Success Story: Vietnam’s Commitment to Containment. Our World in Data. 2021. https://ourworldindata.org/covid-exemplar-vietnam. Accessed 23 Feb 2021.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
