

Recent progress in maintenance treatment of neuromyelitis optica spectrum disorder
- PMID: 33011853
- PMCID: PMC8563615
- DOI: 10.1007/s00415-020-10235-5
Recent progress in maintenance treatment of neuromyelitis optica spectrum disorder
Abstract
Background: Treatment of neuromyelitis optica spectrum disorder (NMOSD) has so far been based on retrospective case series. The results of six randomized clinical trials including five different monoclonal antibodies targeting four molecules and three distinct pathophysiological pathways have recently been published.
Methods: Literature search on clinical trials and case studies in NMOSD up to July 10. 2020.
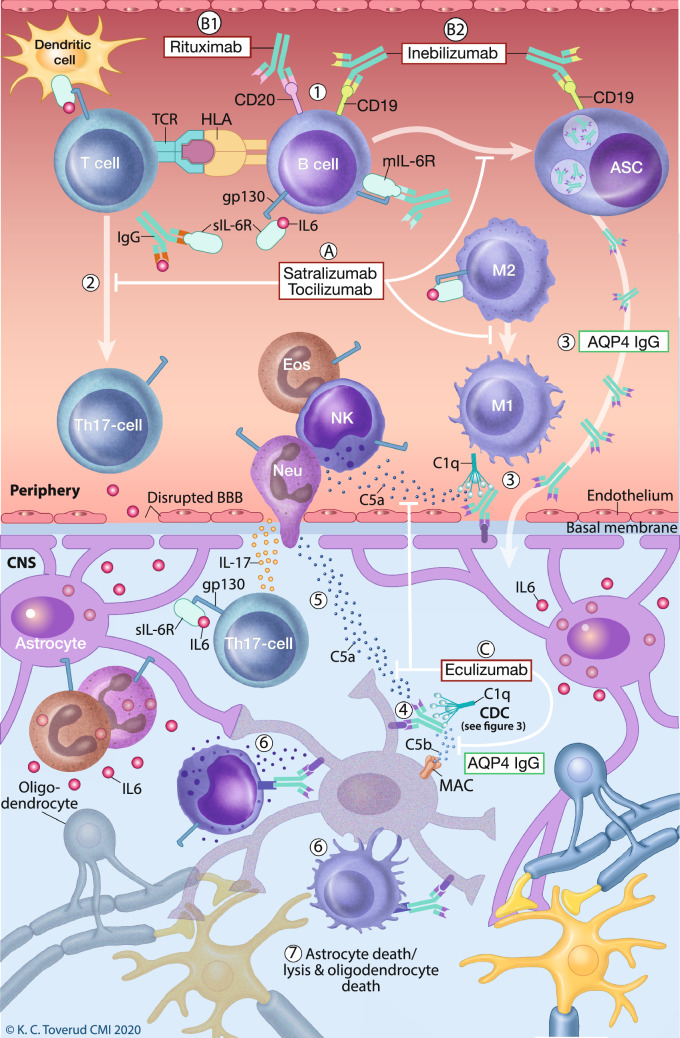
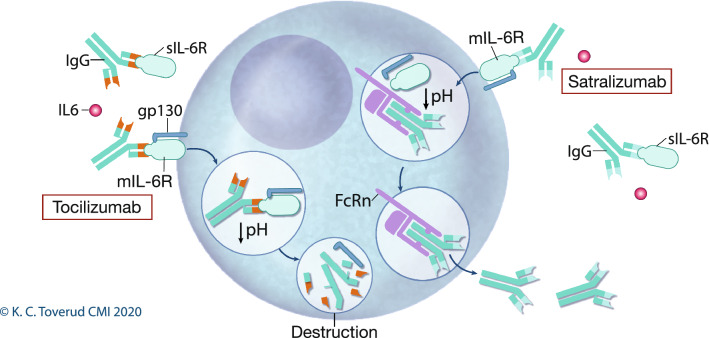
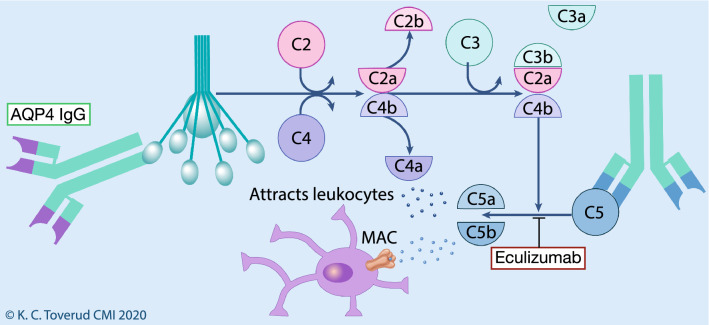
Results: We review mechanism of action, efficacy and side effects, and consequences for reproductive health from traditional immunosuppressants and monoclonal antibodies including rituximab, inebilizumab, eculizumab, tocilizumab and satralizumab.
Conclusion: In NMOSD patients with antibodies against aquaporin 4, monoclonal antibodies that deplete B cells (rituximab and inebilizumab) or interfere with interleukin 6 signaling (tocilizumab and satralizumab) or complement activation (eculizumab) have superior efficacy compared to placebo. Tocilizumab and rituximab were also superior to azathioprine in head-to-head studies. Rituximab, tocilizumab and to some extent eculizumab have well-known safety profiles for other inflammatory diseases, and rituximab and azathioprine may be safe during pregnancy.
Keywords: Demyelinating diseases; Monoclonal antibodies; Neuromyelitis optica spectrum disorder; Treatment.
© 2020. The Author(s).
Conflict of interest statement
Trygve Holmøy has received speakers’ honoraria and/or unrestricted research grants from Biogen, Roche, Sanofi and Merck, and has been principal investigator in studies sponsored by Biogen, Merck and Roche. Rune A. Høglund has received speakers’ honoraria and/or unrestricted grants from Biogen, Merck, Roche and Novartis, and participated as investigator in study sponsored by Roche. Zsolt Illes has received speakers’ honoraria and/or research grants from Biogen, Roche, Sanofi, Novartis and Merck, has been member of advisory boards at Alexion, Biogen, Sanofi, Merck, Roche, Novartis, was member of the adjudication relapse committee in the SAkuraStar and SAkuraSky trials, and has been principal investigator in studies sponsored by Biogen, Merck and Sanofi. Øivind Torkildsen has received speakers’ honoraria and/or unrestricted research grants from Biogen, Roche, Novartis, Merck and Sanofi and has been principal investigator in studies sponsored by Sanofi. Kjell-Morten Myhr has received unrestricted research grants to his institution; scientific advisory board, and speakers’ honoraria from Almirall, Biogen, Genzyme, Merck, Novartis, Roche, or Teva; and has participated in clinical trials organized by Biogen, Merck, Novartis, or Roche.
Figures
Similar articles
-
Effectiveness of treatments in Neuromyelitis optica to modify the course of disease in adult patients. Systematic review of literature.Mult Scler Relat Disord. 2021 May;50:102869. doi: 10.1016/j.msard.2021.102869. Epub 2021 Feb 25. Mult Scler Relat Disord. 2021. PMID: 33711580
-
[Treatment and new evidences in neuromyelitis optica spectrum disorder].Ideggyogy Sz. 2021 Sep 30;74(9-10):309-321. doi: 10.18071/isz.74.0309. Ideggyogy Sz. 2021. PMID: 34657404 Review. Hungarian.
-
Advances in the Treatment of Neuromyelitis Optica Spectrum Disorder.Neurol Clin. 2021 Feb;39(1):35-49. doi: 10.1016/j.ncl.2020.09.003. Epub 2020 Nov 7. Neurol Clin. 2021. PMID: 33223088 Review.
-
Recent advances in the treatment of neuromyelitis optica spectrum disorders.Curr Opin Rheumatol. 2021 May 1;33(3):233-239. doi: 10.1097/BOR.0000000000000791. Curr Opin Rheumatol. 2021. PMID: 33741809 Review.
-
Adverse Events in NMOSD Therapy.Int J Mol Sci. 2022 Apr 9;23(8):4154. doi: 10.3390/ijms23084154. Int J Mol Sci. 2022. PMID: 35456972 Free PMC article. Review.
Cited by
-
Autoantibodies Against the Complement Regulator Factor H in the Serum of Patients With Neuromyelitis Optica Spectrum Disorder.Front Immunol. 2021 Apr 27;12:660382. doi: 10.3389/fimmu.2021.660382. eCollection 2021. Front Immunol. 2021. PMID: 33986750 Free PMC article.
-
Safety and efficacy of interleukin-6-receptor inhibitors in the treatment of neuromyelitis optica spectrum disorders: a meta-analysis.BMC Neurol. 2021 Nov 23;21(1):458. doi: 10.1186/s12883-021-02488-y. BMC Neurol. 2021. PMID: 34814882 Free PMC article.
-
NMOSD-Diagnostic Dilemmas Leading towards Final Diagnosis.Brain Sci. 2022 Jul 6;12(7):885. doi: 10.3390/brainsci12070885. Brain Sci. 2022. PMID: 35884693 Free PMC article.
-
Comparative study of AQP4-NMOSD, MOGAD and seronegative NMOSD: a single-center Belgian cohort.Acta Neurol Belg. 2022 Feb;122(1):135-144. doi: 10.1007/s13760-021-01712-3. Epub 2021 Jun 7. Acta Neurol Belg. 2022. PMID: 34097296 Free PMC article.
-
Aquaporin-4 in Neuromyelitis Optica Spectrum Disorders: A Target of Autoimmunity in the Central Nervous System.Biomolecules. 2022 Apr 17;12(4):591. doi: 10.3390/biom12040591. Biomolecules. 2022. PMID: 35454180 Free PMC article. Review.
References
-
- Lopez-Chiriboga AS, Majed M, Fryer J, Dubey D, McKeon A, Flanagan EP, et al. Association of MOG-IgG serostatus with relapse after acute disseminated encephalomyelitis and proposed diagnostic criteria for MOG-IgG-associated disorders. JAMA Neurol. 2018;75(11):1355–1363. doi: 10.1001/jamaneurol.2018.1814. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
