

Comparison of Centor and McIsaac scores in primary care: a meta-analysis over multiple thresholds
- PMID: 32152041
- PMCID: PMC7065683
- DOI: 10.3399/bjgp20X708833
Comparison of Centor and McIsaac scores in primary care: a meta-analysis over multiple thresholds
Erratum in
-
Correction.Br J Gen Pract. 2020 Apr 30;70(694):230. doi: 10.3399/bjgp20X709565. Print 2020 May. Br J Gen Pract. 2020. PMID: 32354812 Free PMC article. No abstract available.
Abstract
Background: Centor and McIsaac scores are both used to diagnose group A beta-haemolytic streptococcus (GABHS) infection, but have not been compared through meta-analysis.
Aim: To compare the performance of Centor and McIsaac scores at diagnosing patients with GABHS presenting to primary care with pharyngitis.
Design and setting: A meta-analysis of diagnostic test accuracy studies conducted in primary care was performed using a novel model that incorporates data at multiple thresholds.
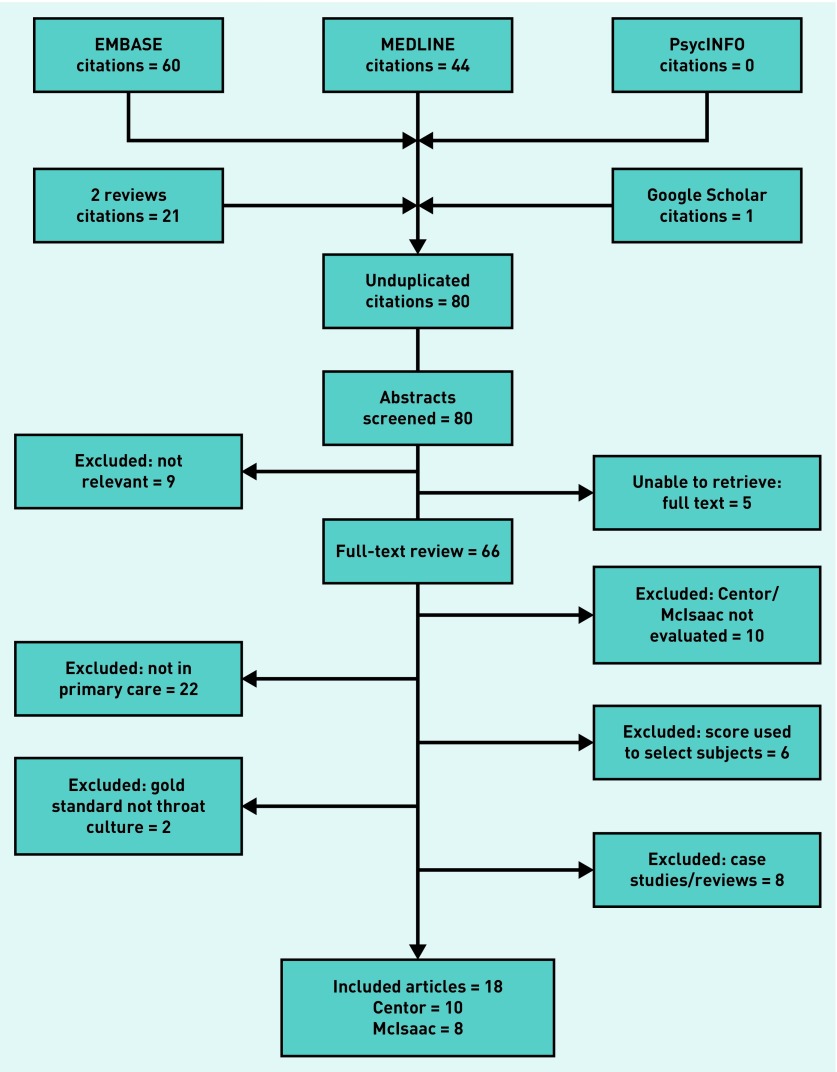
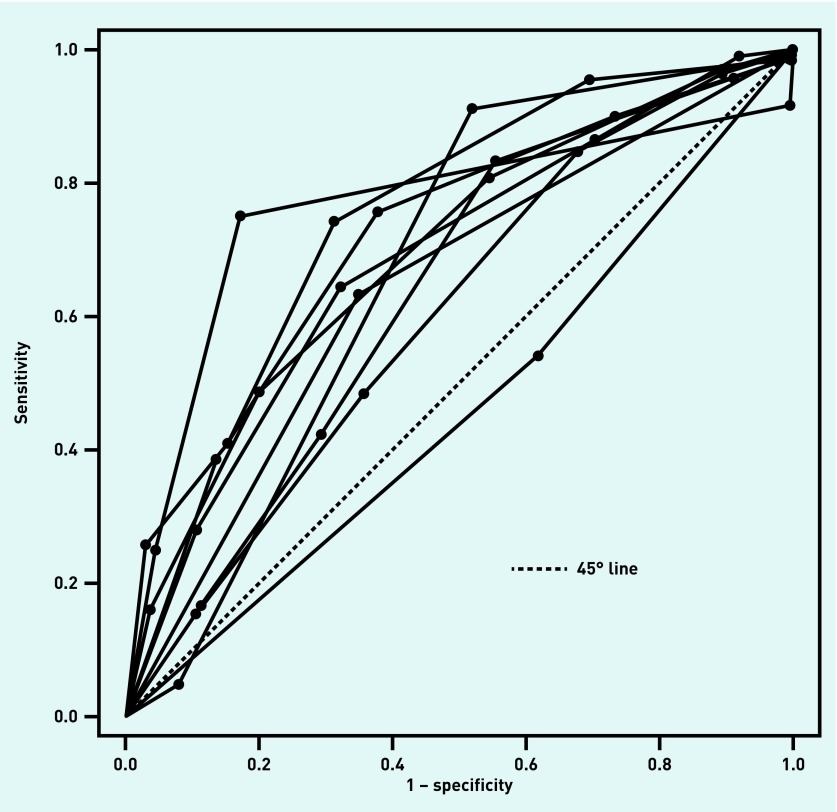
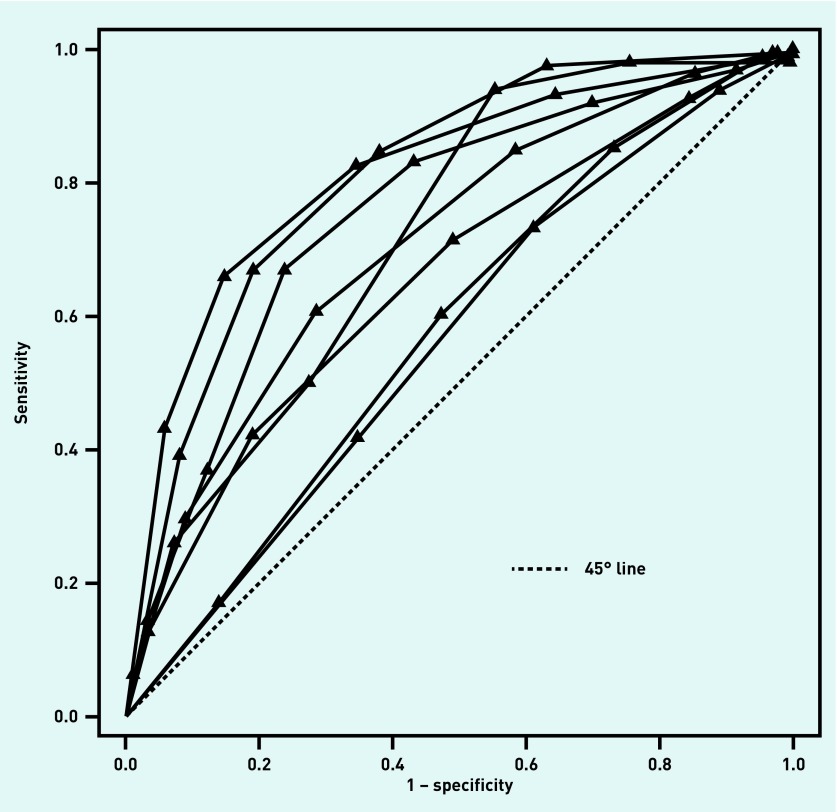
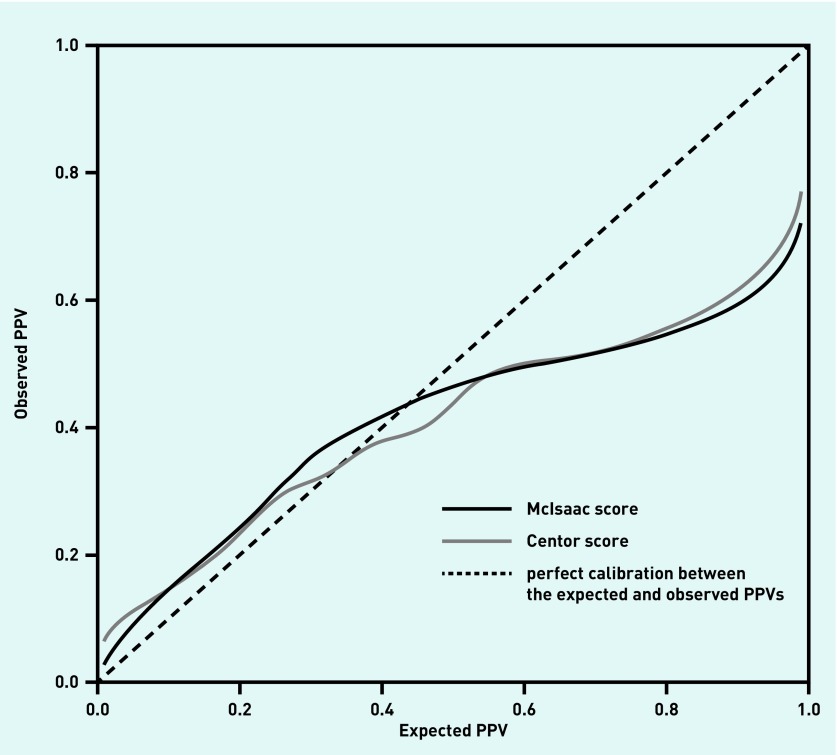
Method: MEDLINE, EMBASE, and PsycINFO were searched for studies published between January 1980 and February 2019. Included studies were: cross-sectional; recruited patients with sore throats from primary care; used the Centor or McIsaac score; had GABHS infection as the target diagnosis; used throat swab culture as the reference standard; and reported 2 × 2 tables across multiple thresholds. Selection and data extraction were conducted by two independent reviewers. QUADAS-2 was used to assess study quality. Summary receiver operating characteristic (SROC) curves were synthesised. Calibration curves were used to assess the transferability of results into practice.
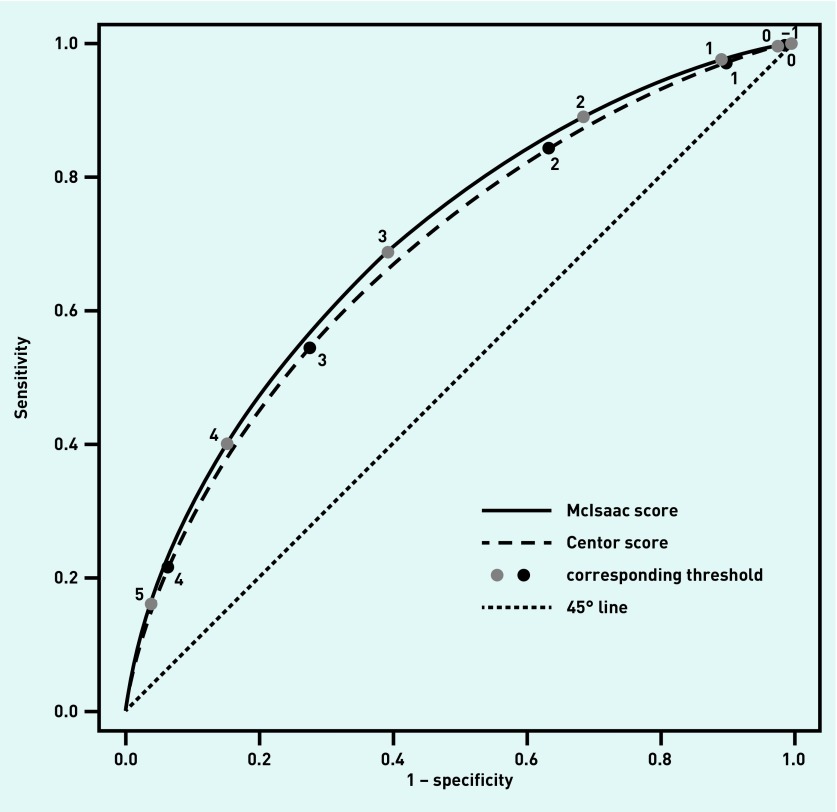
Results: Ten studies using the Centor score and eight using the McIsaac score were included. The prevalence of GABHS ranged between 4% and 44%. The areas under the SROC curves for McIsaac and Centor scores were 0.7052 and 0.6888, respectively. The P-value for the difference (0.0164) was 0.419, suggesting the SROC curves for the tests are equivalent. Both scores demonstrated poor calibration.
Conclusion: Both Centor and McIsaac scores provide only fair discrimination of those with and without GABHS, and appear broadly equivalent in performance. The poor calibration for a positive test result suggests other point-of-care tests are required to rule in GABHS; however, with both Centor and McIsaac scores, a score of ≤0 may be sufficient to rule out infection.
Keywords: Centor score; McIsaac score; diagnosis; meta-analysis; pharyngitis; primary health care.
©The Authors.
Figures
Comment in
-
Clinical scores in primary care.Br J Gen Pract. 2020 Mar 26;70(693):163. doi: 10.3399/bjgp20X708941. Print 2020 Apr. Br J Gen Pract. 2020. PMID: 32217572 Free PMC article. No abstract available.
-
Clinical scores in primary care.Br J Gen Pract. 2020 May 28;70(695):279. doi: 10.3399/bjgp20X709985. Print 2020 Jun. Br J Gen Pract. 2020. PMID: 32467198 Free PMC article. No abstract available.
Similar articles
-
Systematic review and meta-analysis of the accuracy of McIsaac and Centor score in patients presenting to secondary care with pharyngitis.Clin Microbiol Infect. 2024 Apr;30(4):445-452. doi: 10.1016/j.cmi.2023.12.025. Epub 2024 Jan 3. Clin Microbiol Infect. 2024. PMID: 38182052 Review.
-
Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis.Arch Intern Med. 2012 Jun 11;172(11):847-52. doi: 10.1001/archinternmed.2012.950. Arch Intern Med. 2012. PMID: 22566485 Free PMC article.
-
Predicting streptococcal pharyngitis in adults in primary care: a systematic review of the diagnostic accuracy of symptoms and signs and validation of the Centor score.BMC Med. 2011 Jun 1;9:67. doi: 10.1186/1741-7015-9-67. BMC Med. 2011. PMID: 21631919 Free PMC article.
-
Over prescription of antibiotics for adult pharyngitis is prevalent in developing countries but can be reduced using McIsaac modification of Centor scores: a cross-sectional study.BMC Pulm Med. 2012 Nov 24;12:70. doi: 10.1186/1471-2466-12-70. BMC Pulm Med. 2012. PMID: 23176084 Free PMC article.
-
Group A β-hemolytic Streptococcal Pharyngitis: An Updated Review.Curr Pediatr Rev. 2024;21(1):2-17. doi: 10.2174/1573396320666230726145436. Curr Pediatr Rev. 2024. PMID: 37493159 Review.
Cited by
-
Diagnostic accuracy of Fever-PAIN and Centor criteria for bacterial throat infection in adults with sore throat: a secondary analysis of a randomised controlled trial.BJGP Open. 2021 Dec 14;5(6):BJGPO.2021.0122. doi: 10.3399/BJGPO.2021.0122. Print 2021. BJGP Open. 2021. PMID: 34551959 Free PMC article.
-
Amoxicillin vs. placebo to reduce symptoms in children with group A streptococcal pharyngitis: a randomized, multicenter, double-blind, non-inferiority trial.Eur J Pediatr. 2024 Nov;183(11):4773-4782. doi: 10.1007/s00431-024-05705-1. Epub 2024 Aug 31. Eur J Pediatr. 2024. PMID: 39215861 Free PMC article. Clinical Trial.
-
On estimating a constrained bivariate random effects model for meta-analysis of test accuracy studies.Stat Methods Med Res. 2022 Feb;31(2):287-299. doi: 10.1177/09622802211065157. Epub 2022 Jan 7. Stat Methods Med Res. 2022. PMID: 34994667 Free PMC article.
-
Clinical scores in primary care.Br J Gen Pract. 2020 May 28;70(695):279. doi: 10.3399/bjgp20X709985. Print 2020 Jun. Br J Gen Pract. 2020. PMID: 32467198 Free PMC article. No abstract available.
-
Overuse of medical care in paediatrics: A survey from five countries in the European Academy of Pediatrics.Front Pediatr. 2022 Sep 13;10:945540. doi: 10.3389/fped.2022.945540. eCollection 2022. Front Pediatr. 2022. PMID: 36177454 Free PMC article.
References
-
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685–694. - PubMed
-
- Centor RM, Whitherspoon JM, Dalton HP, et al. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1(3):239–246. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical