

Utilization of a breast cancer risk assessment tool by internal medicine residents in a primary care clinic: impact of an educational program
- PMID: 30871497
- PMCID: PMC6416938
- DOI: 10.1186/s12885-019-5418-6
Utilization of a breast cancer risk assessment tool by internal medicine residents in a primary care clinic: impact of an educational program
Abstract
Background: Despite strong evidence of benefit, breast cancer risk assessment and chemoprevention are underutilized by primary care physicians. This study evaluates the impact of an educational program on knowledge and utilization of the NCI Breast Cancer Risk Assessment Tool (BCRAT) by internal medicine residents.
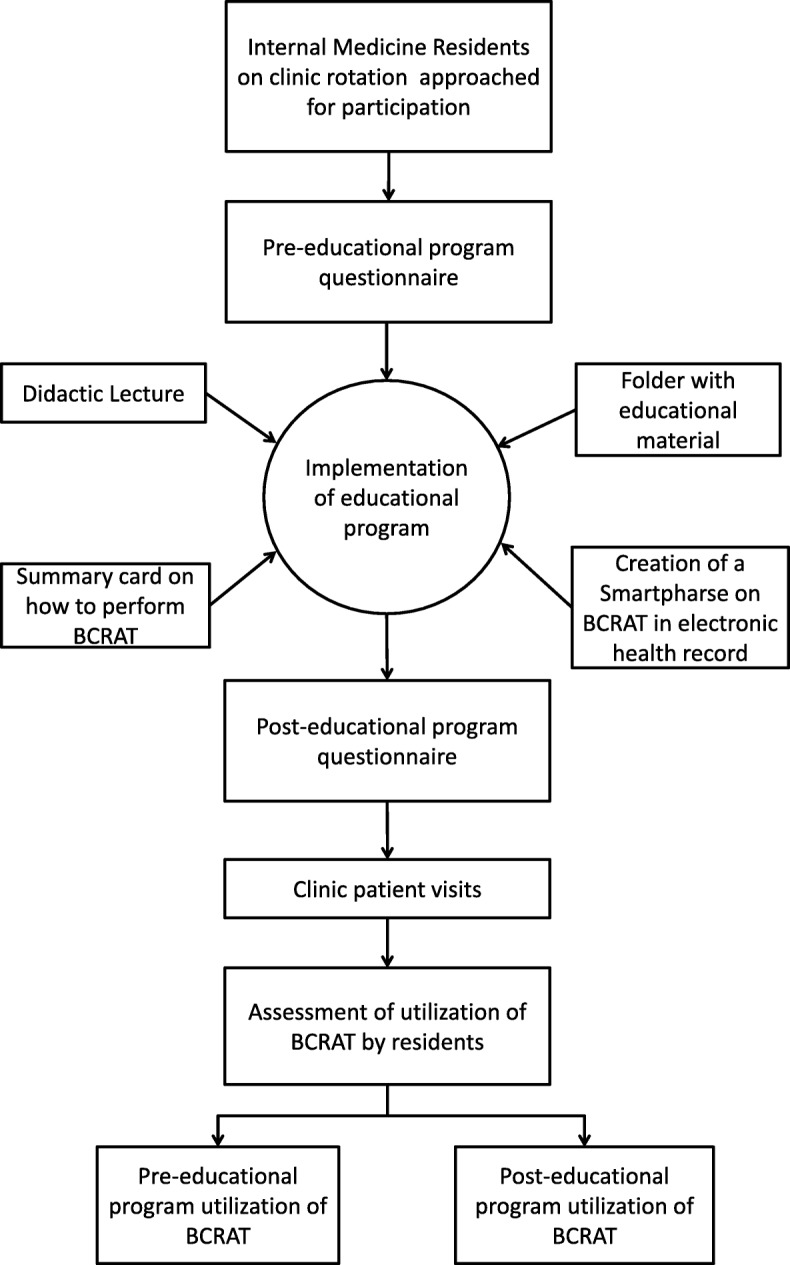
Methods: Internal medicine residents at the primary care clinic at William Beaumont Hospital participated in an educational program on breast cancer risk assessment and chemoprevention. A questionnaire was used to assess knowledge and practice before and after participation. Electronic health records of women between the ages of 35 and 65 who were seen by participating residents for annual health exams between Dec 15, 2015 and Dec 14, 2016 were reviewed. Utilization of BCRAT by the residents was compared pre- and post-educational program.
Results: A total of 43 residents participated in the study. 31 (72.1%) residents reported no prior knowledge about BCRAT. The remaining 12 (27.9%) reported limited knowledge of BCRAT, but the majority of these (n = 10, 83.3%) had not used it in the last six months. For each question on the pre-educational knowledge assessment, fewer than 10% of the residents responded correctly. After implementation of the educational program, there was a significant increase in the proportion of residents who answered correctly (Range: 67 to 100%, p < 0.001). Electronic health records of 301 clinic patients were reviewed, 118 (39.2%) in the pre-educational program group and 183 (60.8%) in the post-educational program group. There was a higher use of BCRAT in the post-educational program group compared to the pre-intervention group (3.8% vs. 0%, p < 0.05). However, a majority (n = 294, 98.7%) of eligible patients from both groups did not undergo breast cancer risk assessment.
Conclusions: Our study demonstrates that an educational intervention improved residents' knowledge of BCRAT. Despite this improvement, a significant proportion of patients did not undergo breast cancer risk assessment. Expanding the scope and duration of this intervention and combining it with innovative use of technology to improve utilization should be the subject of future investigation.
Keywords: BCRAT; Breast Cancer; Chemoprevention; Gail; Internal medicine; Knowledge; Primary care physicians; Residents; Risk assessment.
Conflict of interest statement
Ethics approval and consent to participate
The requirement for informed consent for chart review portion of this study was waived due to retrospective nature of the data. Prior to the participation in the study, resident physicians were provided with an Institutional Review Board-approved written print-out discussing the methodology of the study, the voluntary nature of participation including the option to withdraw from the study at any point, and the contact addresses for further questions and concerns. Since participation into the study and completion of questionnaire was optional for the resident physicians, consent was implied when residents participated in the program and completed the questionnaire. This study was approved by Institutional Review Board at Beaumont Health (HIC-2015-465).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Similar articles
-
Preparing for the primary care clinic: an ambulatory boot camp for internal medicine interns.Med Educ Online. 2015 Nov 24;20:29702. doi: 10.3402/meo.v20.29702. eCollection 2015. Med Educ Online. 2015. PMID: 26609962 Free PMC article.
-
A novel educational strategy to enhance internal medicine residents' familial colorectal cancer knowledge and risk assessment skills.Am J Gastroenterol. 2005 Mar;100(3):677-84. doi: 10.1111/j.1572-0241.2005.41336.x. Am J Gastroenterol. 2005. PMID: 15743368 Clinical Trial.
-
Impact of a competency based curriculum on quality improvement among internal medicine residents.BMC Med Educ. 2014 Nov 28;14:252. doi: 10.1186/s12909-014-0252-7. BMC Med Educ. 2014. PMID: 25429802 Free PMC article.
-
Hospital to home: Improving internal medicine residents' understanding of the needs of older persons after a hospital stay.Acad Med. 2003 Aug;78(8):793-7. doi: 10.1097/00001888-200308000-00009. Acad Med. 2003. PMID: 12915369 Review.
-
[Introducing formative portfolio as a tool for Internal Medicine residents mentoring: review of a pilot project, 2005-2006].Rev Clin Esp. 2008 Oct;208(9):447-54. doi: 10.1157/13127606. Rev Clin Esp. 2008. PMID: 19000473 Review. Spanish.
Cited by
-
A Scoping Review of Personalized, Interactive, Web-Based Clinical Decision Tools Available for Breast Cancer Prevention and Screening in the United States.MDM Policy Pract. 2024 Mar 17;9(1):23814683241236511. doi: 10.1177/23814683241236511. eCollection 2024 Jan-Jun. MDM Policy Pract. 2024. PMID: 38500600 Free PMC article.
-
Synthesis of Existent Oncology Curricula for Primary Care Providers: A Scoping Review With a Global Equity Lens.JCO Glob Oncol. 2023 May;9:e2200298. doi: 10.1200/GO.22.00298. JCO Glob Oncol. 2023. PMID: 37141562 Free PMC article.
-
Cohort profile: design and methods of the Chinese colorectal, breast, lung, liver, and stomach cancer screening trial (C-BLAST).Cancer Biol Med. 2023 Oct 27;20(10):713-20. doi: 10.20892/j.issn.2095-3941.2023.0278. Cancer Biol Med. 2023. PMID: 37905555 Free PMC article. No abstract available.
-
A streamlined model for use in clinical breast cancer risk assessment maintains predictive power and is further improved with inclusion of a polygenic risk score.PLoS One. 2021 Jan 22;16(1):e0245375. doi: 10.1371/journal.pone.0245375. eCollection 2021. PLoS One. 2021. PMID: 33481864 Free PMC article.
-
Assessment of common risk factors and validation of the Gail model for breast cancer: A hospital-based study from Western India.Tzu Chi Med J. 2020 Apr 10;32(4):362-366. doi: 10.4103/tcmj.tcmj_171_19. eCollection 2020 Oct-Dec. Tzu Chi Med J. 2020. PMID: 33163382 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
