

Second-line rescue treatment of Helicobacter pylori infection: Where are we now?
- PMID: 30386104
- PMCID: PMC6209570
- DOI: 10.3748/wjg.v24.i40.4548
Second-line rescue treatment of Helicobacter pylori infection: Where are we now?
Abstract
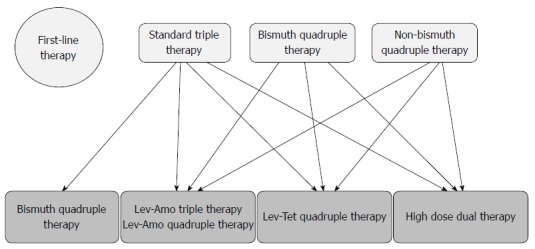
At present, the best rescue therapy for Helicobacter pylori (H. pylori) infection following failure of first-line eradication remains unclear. The Maastricht V/Florence Consensus Report recommends bismuth quadruple therapy, or fluoroquinolone-amoxicillin triple/quadruple therapy as the second-line therapy for H. pylori infection. Meta-analyses have shown that bismuth quadruple therapy and levofloxacin-amoxicillin triple therapy have comparable eradication rates, while the former has more adverse effects than the latter. There are no significant differences between the eradication rates of levofloxacin-amoxicillin triple and quadruple therapies. However, the eradication rates of both levofloxacin-containing treatments are suboptimal. An important caveat of levofloxacin-amoxicillin triple or quadruple therapy is poor eradication efficacy in the presence of fluoroquinolone resistance. High-dose dual therapy is an emerging second-line therapy and has an eradication efficacy comparable with levofloxacin-amoxicillin triple therapy. Recently, a 10-d tetracycline-levofloxacin (TL) quadruple therapy comprised of a proton pump inhibitor, bismuth, tetracycline and levofloxacin has been developed, which achieves a markedly higher eradication rate compared with levofloxacin-amoxicillin triple therapy (98% vs 69%) in patients with failure of standard triple, bismuth quadruple or non-bismuth quadruple therapy. The present article reviews current second-line anti-H. pylori regimens and treatment algorisms. In conclusion, bismuth quadruple therapy, levofloxacin-amoxicillin triple/quadruple therapy, high-dose dual therapy and TL quadruple therapy can be used as second-line treatment for H. pylori infection. Current evidence suggests that 10-d TL quadruple therapy is a simple and effective regimen, and has the potential to become a universal rescue treatment following eradication failure by all first-line eradication regimens for H. pylori infection.
Keywords: Bismuth quadruple therapy; Helicobacter pylori; High-dose dual therapy; Levofloxacin-amoxicillin triple therapy; Rescue treatment; Tetracycline-levofloxacin quadruple therapy.
Conflict of interest statement
Conflict-of-interest statement: Both authors have no conflicts of interest.
Figures
Similar articles
-
Ten-Day Quadruple Therapy Comprising Proton Pump Inhibitor, Bismuth, Tetracycline, and Levofloxacin is More Effective than Standard Levofloxacin Triple Therapy in the Second-Line Treatment of Helicobacter pylori Infection: A Randomized Controlled Trial.Am J Gastroenterol. 2017 Sep;112(9):1374-1381. doi: 10.1038/ajg.2017.195. Epub 2017 Jul 18. Am J Gastroenterol. 2017. PMID: 28719592 Clinical Trial.
-
Tetracycline-levofloxacin versus amoxicillin-levofloxacin quadruple therapies in the second-line treatment of Helicobacter pylori infection.Helicobacter. 2021 Oct;26(5):e12840. doi: 10.1111/hel.12840. Epub 2021 Aug 12. Helicobacter. 2021. PMID: 34390083 Clinical Trial.
-
Helicobacter pylori second-line rescue therapy with levofloxacin- and bismuth-containing quadruple therapy, after failure of standard triple or non-bismuth quadruple treatments.Aliment Pharmacol Ther. 2015 Apr;41(8):768-75. doi: 10.1111/apt.13128. Epub 2015 Feb 23. Aliment Pharmacol Ther. 2015. PMID: 25703120 Clinical Trial.
-
Update on the second-line treatment of Helicobacter pylori infection: a narrative review.Therap Adv Gastroenterol. 2023 Sep 4;16:17562848231192750. doi: 10.1177/17562848231192750. eCollection 2023. Therap Adv Gastroenterol. 2023. PMID: 37675247 Free PMC article. Review.
-
Novel and Effective Therapeutic Regimens for Helicobacter pylori in an Era of Increasing Antibiotic Resistance.Front Cell Infect Microbiol. 2017 May 5;7:168. doi: 10.3389/fcimb.2017.00168. eCollection 2017. Front Cell Infect Microbiol. 2017. PMID: 28529929 Free PMC article. Review.
Cited by
-
Eradication rate and safety of a "simplified rescue therapy": 14-day vonoprazan and amoxicillin dual regimen as rescue therapy on treatment of Helicobacter pylori infection previously failed in eradication: A real-world, retrospective clinical study in China.Helicobacter. 2022 Oct;27(5):e12918. doi: 10.1111/hel.12918. Epub 2022 Jul 25. Helicobacter. 2022. PMID: 35877765 Free PMC article.
-
Efficacy and tolerability of Helicobacter pylori eradication regimes in South Kivu, Eastern of the Democratic Republic of Congo: A single center observational study.Health Sci Rep. 2024 Mar 7;7(3):e1960. doi: 10.1002/hsr2.1960. eCollection 2024 Mar. Health Sci Rep. 2024. PMID: 38455644 Free PMC article.
-
Efficacy and safety of modified tetracycline dosing in a quadruple therapy for Helicobacter pylori: A retrospective single center study.World J Gastroenterol. 2023 Jun 14;29(22):3508-3518. doi: 10.3748/wjg.v29.i22.3508. World J Gastroenterol. 2023. PMID: 37389237 Free PMC article.
-
Molecular mechanism of Helicobacter pylori-induced autophagy in gastric cancer.Oncol Lett. 2019 Dec;18(6):6221-6227. doi: 10.3892/ol.2019.10976. Epub 2019 Oct 10. Oncol Lett. 2019. PMID: 31788098 Free PMC article. Review.
-
Helicobacter pylori in the post-antibiotics era: from virulence factors to new drug targets and therapeutic agents.Arch Microbiol. 2023 Aug 7;205(9):301. doi: 10.1007/s00203-023-03639-0. Arch Microbiol. 2023. PMID: 37550555 Free PMC article. Review.
References
-
- Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med. 2002;347:1175–1186. - PubMed
-
- Zucca E, Dreyling M; ESMO Guidelines Working Group. Gastric marginal zone lymphoma of MALT type: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20 Suppl 4:113–114. - PubMed
-
- Gatta L, Vakil N, Leandro G, Di Mario F, Vaira D. Sequential therapy or triple therapy for Helicobacter pylori infection: systematic review and meta-analysis of randomized controlled trials in adults and children. Am J Gastroenterol. 2009;104:3069–79; quiz 1080. - PubMed
-
- Hsu PI, Wu DC, Wu JY, Graham DY. Is there a benefit to extending the duration of Helicobacter pylori sequential therapy to 14 days? Helicobacter. 2011;16:146–152. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
