

Quizartinib, an FLT3 inhibitor, as monotherapy in patients with relapsed or refractory acute myeloid leukaemia: an open-label, multicentre, single-arm, phase 2 trial
- PMID: 29859851
- PMCID: PMC8152787
- DOI: 10.1016/S1470-2045(18)30240-7
Quizartinib, an FLT3 inhibitor, as monotherapy in patients with relapsed or refractory acute myeloid leukaemia: an open-label, multicentre, single-arm, phase 2 trial
Abstract
Background: Old age and FMS-like tyrosine kinase 3 internal tandem duplication (FLT3-ITD) mutations in patients with acute myeloid leukaemia are associated with early relapse and poor survival. Quizartinib is an oral, highly potent, and selective next-generation FLT3 inhibitor with clinical antileukaemic activity in relapsed or refractory acute myeloid leukaemia. We aimed to assess the efficacy and safety of single-agent quizartinib in patients with relapsed or refractory acute myeloid leukaemia.
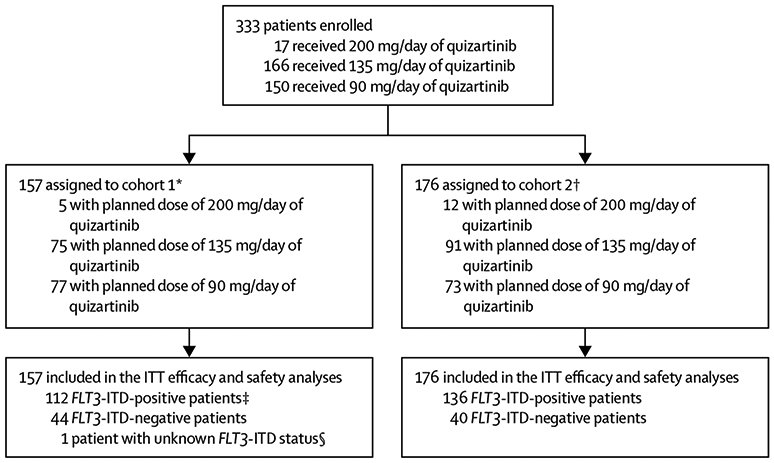
Methods: We did an open-label, multicentre, single-arm, phase 2 trial at 76 hospitals and cancer centres in the USA, Europe, and Canada. We enrolled patients with morphologically documented primary acute myeloid leukaemia or acute myeloid leukaemia secondary to myelodysplastic syndromes and an Eastern Cooperative Oncology Group (ECOG) performance status of 0-2 into two predefined, independent cohorts: patients who were aged 60 years or older with relapsed or refractory acute myeloid leukaemia within 1 year after first-line therapy (cohort 1), and those who were 18 years or older with relapsed or refractory disease following salvage chemotherapy or haemopoietic stem cell transplantation (cohort 2). Patients with an FLT3-ITD allelic frequency of more than 10% were considered as FLT3-ITD positive, whereas all other patients were considered as FLT3-ITD negative. Patients received quizartinib once daily as an oral solution; the initial 17 patients received 200 mg per day but the QTcF interval was prolonged for more than 60 ms above baseline in some of these patients. Subsequently, doses were amended for all patients to 135 mg per day for men and 90 mg per day for women. The co-primary endpoints were the proportion of patients who achieved a composite complete remission (defined as complete remission + complete remission with incomplete platelet recovery + complete remission with incomplete haematological recovery) and the proportion of patients who achieved a complete remission. Efficacy and safety analyses included all patients who received at least one dose of quizartinib (ie, the intention-to-treat population). Patients with a locally assessed post-treatment bone marrow aspirate or biopsy were included in efficacy analyses by response; all other patients were considered to have an unknown response. This study is registered with ClinicalTrials.gov, number NCT00989261, and with the European Clinical Trials Database, EudraCT 2009-013093-41, and is completed.
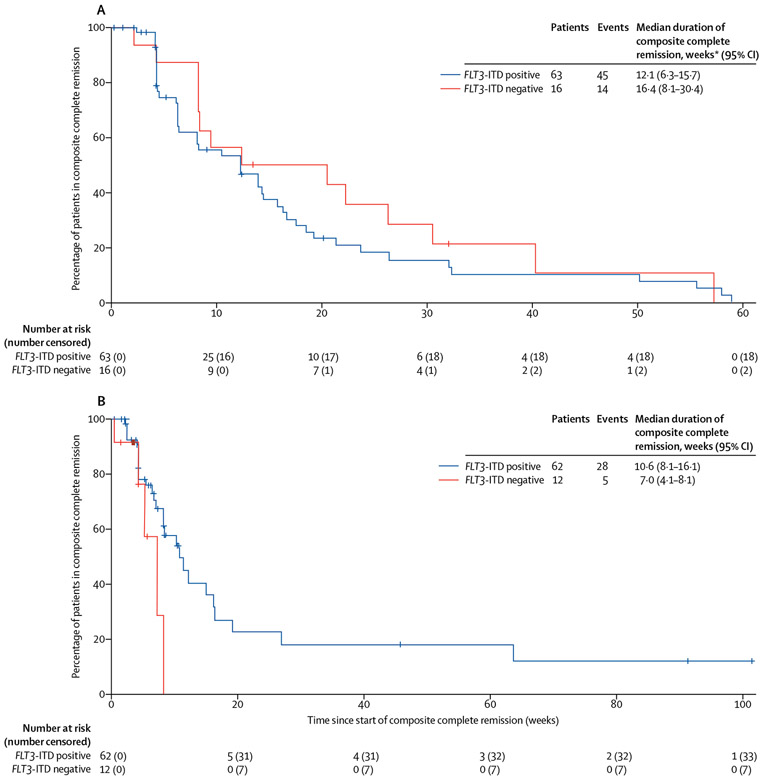
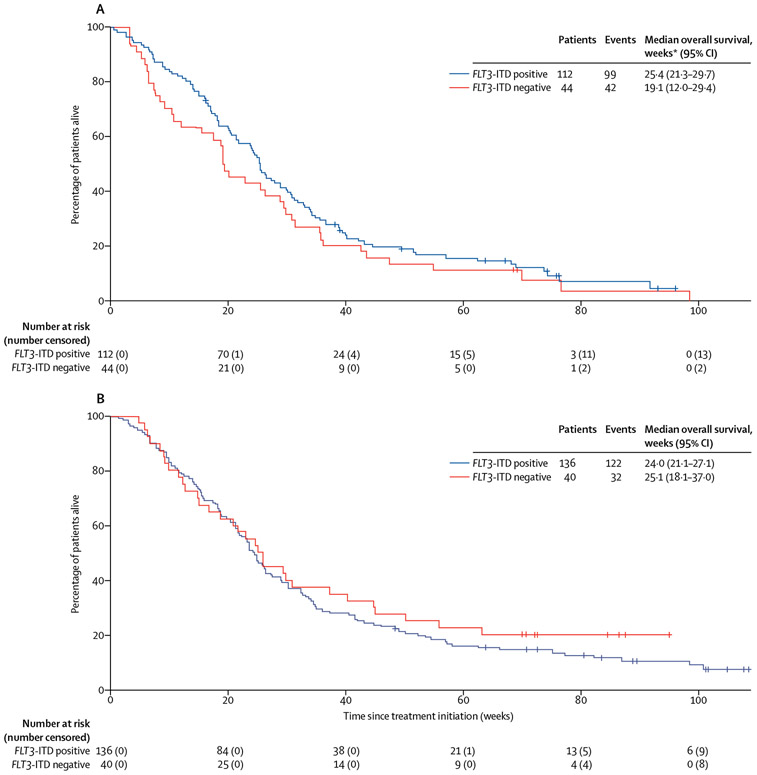
Findings: Between Nov 19, 2009, and Oct 31, 2011, a total of 333 patients were enrolled (157 in cohort 1 and 176 in cohort 2). In cohort 1, 63 (56%) of 112 FLT3-ITD-positive patients and 16 (36%) of 44 FLT3-ITD-negative patients achieved composite complete remission, with three (3%) FLT3-ITD-positive patients and two (5%) FLT3-ITD-negative patients achieving complete remission. In cohort 2, 62 (46%) of 136 FLT3-ITD-positive patients achieved composite complete remission with five (4%) achieving complete remission, whereas 12 (30%) of 40 FLT3-ITD-negative patients achieved composite complete remission with one (3%) achieving complete remission. Across both cohorts (ie, the intention-to-treat population of 333 patients), grade 3 or worse treatment-related treatment-emergent adverse events in 5% or more of patients were febrile neutropenia (76 [23%] of 333), anaemia (75 [23%]), thrombocytopenia (39 [12%]), QT interval corrected using Fridericia's formula (QTcF) prolongation (33 [10%]), neutropenia (31 [9%]), leucopenia (22 [7%]), decreased platelet count (20 [6%]), and pneumonia (17 [5%]). Serious adverse events occurring in 5% or more of patients were febrile neutropenia (126 [38%] of 333; 76 treatment related), acute myeloid leukaemia progression (73 [22%]), pneumonia (40 [12%]; 14 treatment related), QTcF prolongation (33 [10%]; 32 treatment related), sepsis (25 [8%]; eight treatment related), and pyrexia (18 [5%]; nine treatment related). Notable serious adverse events occurring in less than 5% of patients were torsades de pointes (one [<1%]) and hepatic failure (two [1%]). In total, 125 (38%) of 333 patients died within the study treatment period, including the 30-day follow-up. 18 (5%) patients died because of an adverse event considered by the investigator to be treatment related (ten [6%] of 157 patients in cohort 1 and eight [5%] of 176 in cohort 2.
Interpretation: Single-agent quizartinib was shown to be highly active and generally well tolerated in patients with relapsed or refractory acute myeloid leukaemia, particularly those with FLT3-ITD mutations. These findings confirm that targeting the FLT3-ITD driver mutation with a highly potent and selective FLT3 inhibitor is a promising clinical strategy to help improve clinical outcomes in patients with very few options. Phase 3 studies (NCT02039726; NCT02668653) will examine quizartinib at lower starting doses.
Funding: Ambit Biosciences/Daiichi Sankyo.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
JC has received grants and personal fees from Astellas/Daiichi Sankyo during the conduct of this study; grants and personal fees from Astellas, Ariad, and Novartis; and grants from Arog Pharmaceuticals and Forma Therapeutics outside the submitted work. AEP has received personal fees and non-financial support from Ambit Biosciences/Daiichi Sankyo, Astellas US Pharma, Arog Pharmaceuticals, and Novartis outside the submitted work. HDoh has received grants and personal fees from Novartis and grants from Arog Pharmaceuticals outside the submitted work. BS has received other fees from Ambit Biosciences/Daiichi Sankyo during the conduct of this study and non-financial support from Novartis Pharma AG, Amgen GmbH, GlaxoSmithKline GmbH, PharmaMar, and Astellas Pharma GmbH outside the submitted work. HDom has received personal fees from Ambit Biosciences/Daiichi Sankyo during the conduct of this study; grants and personal fees from Roche/Genentech, Amgen, Ariad, Jazz Pharma, and Kite Pharma; and personal fees from Pfizer, Novartis, Celgene, Agios, Sunesis, Karyopharm, Menarini, Astellas, Janssen, Servier, and Seattle Genetics outside the submitted work. SS has received personal fees from Astellas, Daiichi Sankyo, Novartis, and Sunesis; and other fees from Alexion, Boehringer Ingelheim, CTI Biopharma, Baxalta, Sunesis, and Tolero outside the submitted work. JKA has received non-financial support from Northwestern University during the conduct of this study; personal fees from Immune Pharmaceuticals and Celgene; personal and other fees from Syros, Janssen Pharmaceuticals, NCCN, Novartis, Seattle Genetics, Spectrum, BMS, and Ariad; and other fees from MethylGene, Boehringer Ingelheim, Astellas, Agios Pharmaceuticals, CSL, Cyclacel, Epizyme, Genentech, Pfizer, BioLineRX, and Talon Therapeutics outside the submitted work. NR has received non-financial support from Merck Sharp & Dohme and personal fees from Jazz Pharmaceuticals, Sunesis, Novartis, and Pfizer outside the submitted work. NPS has received grants from Ambit Biosciences/Daiichi Sankyo during the conduct of this study. CCS has received grants from Astellas during the conduct of this study. GG and DT are former employees of Ambit Biosciences/ Daiichi Sankyo. DL has received personal fees from Daiichi Sankyo during the conduct of this study, and personal fees and other fees from Daiichi Sankyo outside the submitted work. ML has received grants from the National Cancer Institute, USA, during the conduct of this study and served as a consultant for Astellas, Daiichi Sankyo, Novartis, and Arog Pharmaceuticals outside the submitted work. HK, GM, TK, PR, EE, CDB, AB, AK, ESW, and NI declare no competing interests.
Figures
Comment in
-
FLT3 inhibitors for relapsed or refractory acute myeloid leukaemia.Lancet Oncol. 2018 Jul;19(7):849-850. doi: 10.1016/S1470-2045(18)30335-8. Epub 2018 May 31. Lancet Oncol. 2018. PMID: 29859852 No abstract available.
Similar articles
-
Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): a multicentre, randomised, controlled, open-label, phase 3 trial.Lancet Oncol. 2019 Jul;20(7):984-997. doi: 10.1016/S1470-2045(19)30150-0. Epub 2019 Jun 4. Lancet Oncol. 2019. PMID: 31175001 Clinical Trial.
-
Selective inhibition of FLT3 by gilteritinib in relapsed or refractory acute myeloid leukaemia: a multicentre, first-in-human, open-label, phase 1-2 study.Lancet Oncol. 2017 Aug;18(8):1061-1075. doi: 10.1016/S1470-2045(17)30416-3. Epub 2017 Jun 20. Lancet Oncol. 2017. PMID: 28645776 Free PMC article. Clinical Trial.
-
Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): a randomised, double-blind, placebo-controlled, phase 3 trial.Lancet. 2023 May 13;401(10388):1571-1583. doi: 10.1016/S0140-6736(23)00464-6. Epub 2023 Apr 25. Lancet. 2023. PMID: 37116523 Clinical Trial.
-
Practical Considerations for Treatment of Relapsed/Refractory FLT3-ITD Acute Myeloid Leukaemia with Quizartinib: Illustrative Case Reports.Clin Drug Investig. 2020 Mar;40(3):227-235. doi: 10.1007/s40261-019-00881-7. Clin Drug Investig. 2020. PMID: 31912423 Free PMC article. Review.
-
Quizartinib in the treatment of FLT3-internal-tandem duplication-positive acute myeloid leukemia.Future Oncol. 2019 Dec;15(34):3885-3894. doi: 10.2217/fon-2019-0353. Epub 2019 Sep 27. Future Oncol. 2019. PMID: 31559849 Review.
Cited by
-
Small molecules in targeted cancer therapy: advances, challenges, and future perspectives.Signal Transduct Target Ther. 2021 May 31;6(1):201. doi: 10.1038/s41392-021-00572-w. Signal Transduct Target Ther. 2021. PMID: 34054126 Free PMC article. Review.
-
Targeting Tyrosine Kinases in Acute Myeloid Leukemia: Why, Who and How?Int J Mol Sci. 2019 Jul 12;20(14):3429. doi: 10.3390/ijms20143429. Int J Mol Sci. 2019. PMID: 31336846 Free PMC article. Review.
-
Current and Emerging Therapies for Acute Myeloid Leukemia.Cancer Treat Res. 2021;181:57-73. doi: 10.1007/978-3-030-78311-2_4. Cancer Treat Res. 2021. PMID: 34626355
-
Efficacy and Synergy of Small Molecule Inhibitors Targeting FLT3-ITD+ Acute Myeloid Leukemia.Cancers (Basel). 2021 Dec 8;13(24):6181. doi: 10.3390/cancers13246181. Cancers (Basel). 2021. PMID: 34944800 Free PMC article.
-
Overcoming Resistance to FLT3 Inhibitors in the Treatment of FLT3-Mutated AML.Int J Mol Sci. 2020 Feb 24;21(4):1537. doi: 10.3390/ijms21041537. Int J Mol Sci. 2020. PMID: 32102366 Free PMC article. Review.
References
-
- Levis M, Small D. FLT3: ITDoes matter in leukemia. Leukemia 2003; 17: 1738–52. - PubMed
-
- Boissel N, Cayuela JM, Preudhomme C, et al. Prognostic significance of FLT3 internal tandem repeat in patients with de novo acute myeloid leukemia treated with reinforced courses of chemotherapy. Leukemia 2002; 16: 1699–704. - PubMed
-
- Whitman SP, Maharry K, Radmacher MD, et al. FLT3 internal tandem duplication associates with adverse outcome and gene-and microRNA-expression signatures in patients 60 years of age or older with primary cytogenetically normal acute myeloid leukemia: a Cancer and Leukemia Group B study. Blood 2010; 116: 3622–26. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
