

Ocular congenital cranial dysinnervation disorders (CCDDs): insights into axon growth and guidance
- PMID: 28459979
- PMCID: PMC5886468
- DOI: 10.1093/hmg/ddx168
Ocular congenital cranial dysinnervation disorders (CCDDs): insights into axon growth and guidance
Abstract
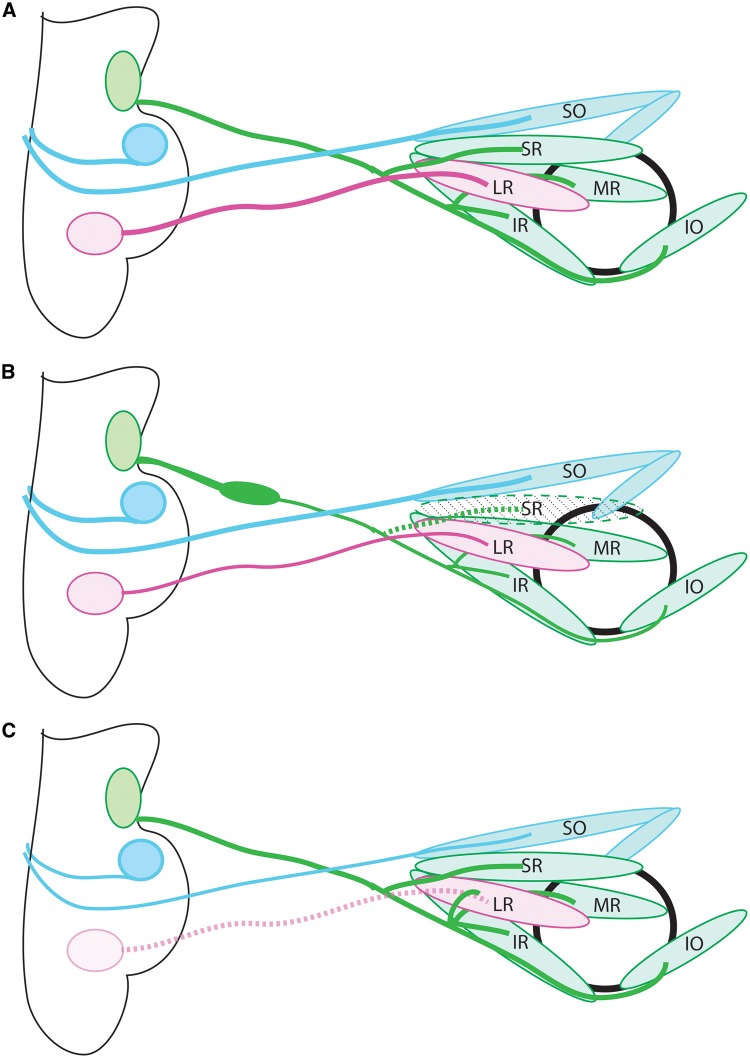
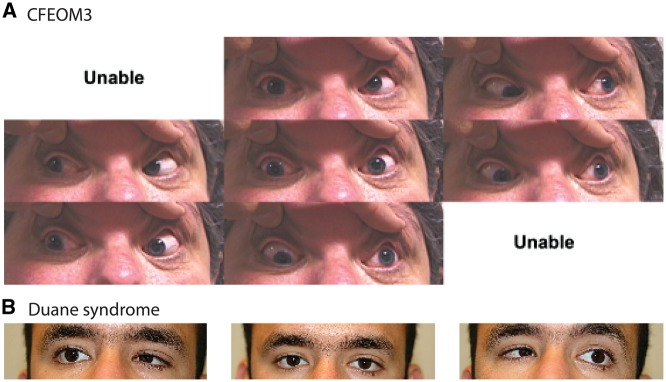
Unraveling the genetics of the paralytic strabismus syndromes known as congenital cranial dysinnervation disorders (CCDDs) is both informing physicians and their patients and broadening our understanding of development of the ocular motor system. Genetic mutations underlying ocular CCDDs alter either motor neuron specification or motor nerve development, and highlight the importance of modulations of cell signaling, cytoskeletal transport, and microtubule dynamics for axon growth and guidance. Here we review recent advances in our understanding of two CCDDs, congenital fibrosis of the extraocular muscles (CFEOM) and Duane retraction syndrome (DRS), and discuss what they have taught us about mechanisms of axon guidance and selective vulnerability. CFEOM presents with congenital ptosis and restricted eye movements, and can be caused by heterozygous missense mutations in the kinesin motor protein KIF21A or in the β-tubulin isotypes TUBB3 or TUBB2B. CFEOM-causing mutations in these genes alter protein function and result in axon growth and guidance defects. DRS presents with inability to abduct one or both eyes. It can be caused by decreased function of several transcription factors critical for abducens motor neuron identity, including MAFB, or by heterozygous missense mutations in CHN1, which encodes α2-chimaerin, a Rac-GAP GTPase that affects cytoskeletal dynamics. Examination of the orbital innervation in mice lacking Mafb has established that the stereotypical misinnervation of the lateral rectus by fibers of the oculomotor nerve in DRS is secondary to absence of the abducens nerve. Studies of a CHN1 mouse model have begun to elucidate mechanisms of selective vulnerability in the nervous system.
© The Author 2017. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
An inherited TUBB2B mutation alters a kinesin-binding site and causes polymicrogyria, CFEOM and axon dysinnervation.Hum Mol Genet. 2012 Dec 15;21(26):5484-99. doi: 10.1093/hmg/dds393. Epub 2012 Sep 21. Hum Mol Genet. 2012. PMID: 23001566 Free PMC article.
-
Clinical and genetic characteristics of Chinese patients with congenital cranial dysinnervation disorders.Orphanet J Rare Dis. 2022 Dec 9;17(1):431. doi: 10.1186/s13023-022-02582-5. Orphanet J Rare Dis. 2022. PMID: 36494820 Free PMC article.
-
Optic Nerve Head and Retinal Abnormalities Associated with Congenital Fibrosis of the Extraocular Muscles.Int J Mol Sci. 2021 Mar 4;22(5):2575. doi: 10.3390/ijms22052575. Int J Mol Sci. 2021. PMID: 33806565 Free PMC article.
-
[Congenital fibrosis of extraocular muscles (CFEOM) and other phenotypes of congenital cranial dysinnervation syndromes (CCDD)].Nervenarzt. 2005 Apr;76(4):395-402. doi: 10.1007/s00115-004-1742-3. Nervenarzt. 2005. PMID: 15221064 Review. German.
-
Applications of molecular genetics to the understanding of congenital ocular motility disorders.Ann N Y Acad Sci. 2002 Apr;956:55-63. doi: 10.1111/j.1749-6632.2002.tb02808.x. Ann N Y Acad Sci. 2002. PMID: 11960793 Review.
Cited by
-
Kif21a deficiency leads to impaired glomerular filtration barrier function.Sci Rep. 2023 Nov 6;13(1):19161. doi: 10.1038/s41598-023-46270-1. Sci Rep. 2023. PMID: 37932480 Free PMC article.
-
Axonal Growth Abnormalities Underlying Ocular Cranial Nerve Disorders.Annu Rev Vis Sci. 2021 Sep 15;7:827-850. doi: 10.1146/annurev-vision-093019-114307. Epub 2021 Jun 3. Annu Rev Vis Sci. 2021. PMID: 34081534 Free PMC article. Review.
-
Two novel CHN1 variants identified in Duane retraction syndrome pedigrees disrupt development of ocular motor nerves in zebrafish.J Hum Genet. 2024 Jan;69(1):33-39. doi: 10.1038/s10038-023-01201-w. Epub 2023 Oct 18. J Hum Genet. 2024. PMID: 37853116
-
The Rac-GAP alpha2-Chimaerin Signals via CRMP2 and Stathmins in the Development of the Ocular Motor System.J Neurosci. 2021 Aug 4;41(31):6652-6672. doi: 10.1523/JNEUROSCI.0983-19.2021. Epub 2021 Jun 24. J Neurosci. 2021. PMID: 34168008 Free PMC article.
-
Expanding the genetics and phenotypes of ocular congenital cranial dysinnervation disorders.medRxiv [Preprint]. 2024 Mar 26:2024.03.22.24304594. doi: 10.1101/2024.03.22.24304594. medRxiv. 2024. Update in: Genet Med. 2024 Jul 18;27(4):101216. doi: 10.1016/j.gim.2024.101216. PMID: 38585811 Free PMC article. Updated. Preprint.
References
-
- Gutowski N.J., Bosley T.M., Engle E.C. (2003) 110th ENMC International Workshop: the congenital cranial dysinnervation disorders (CCDDs). Naarden, The Netherlands, 25–27 October, 2002. Neuromuscul. Disord., 13, 573–578. - PubMed
-
- Engle E.C. (2002) The molecular basis of the congenital fibrosis syndromes. Strabismus, 10, 125–128. - PubMed
-
- Heidary G., Engle E.C., Hunter D.G. (2008) Congenital fibrosis of the extraocular muscles. Semin. Ophthalmol., 23, 3–8. - PubMed
-
- Bienfang D.C. (1975) Crossing axons in the third nerve nucleus. Invest. Ophthalmol., 14, 927–931. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
