

Fibrous dysplasia of bone: craniofacial and dental implications
- PMID: 27493082
- PMCID: PMC5292317
- DOI: 10.1111/odi.12563
Fibrous dysplasia of bone: craniofacial and dental implications
Abstract
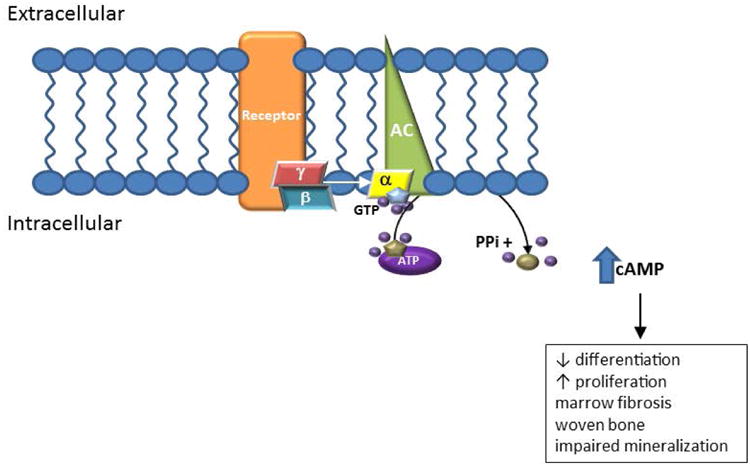
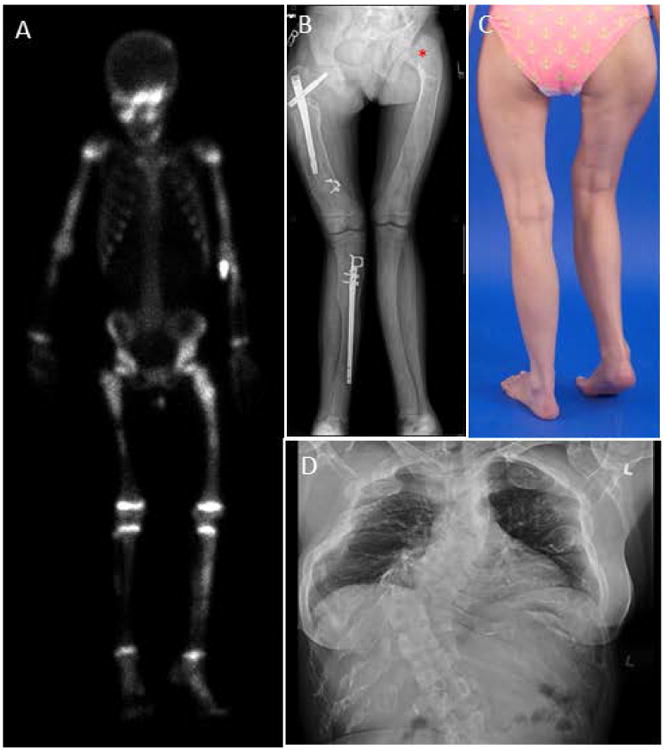
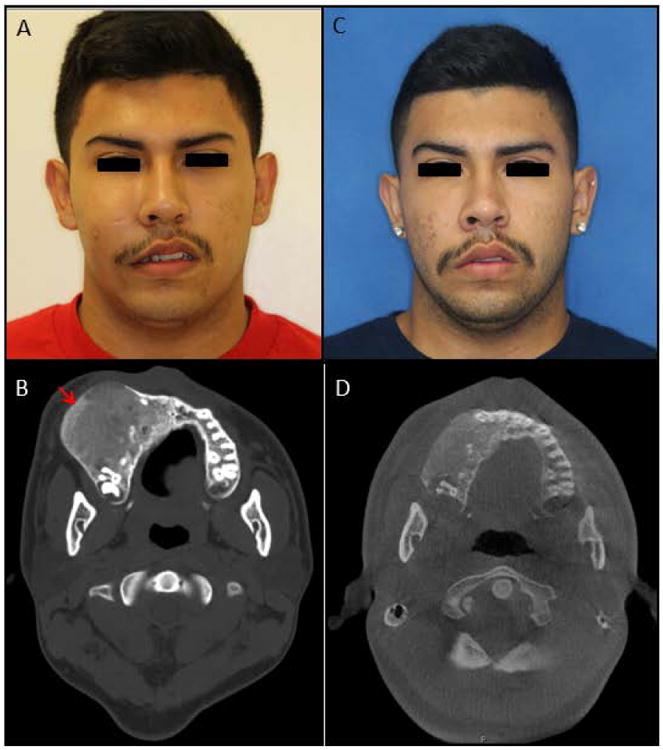
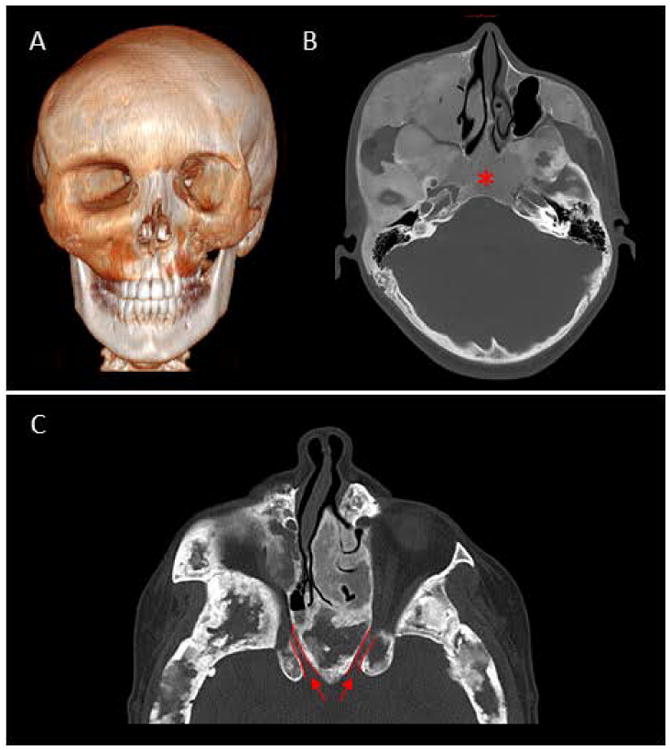
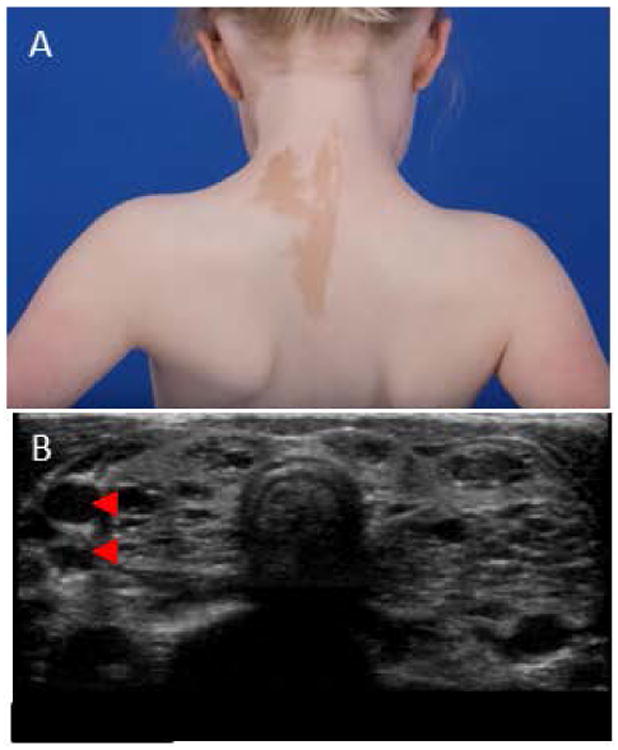
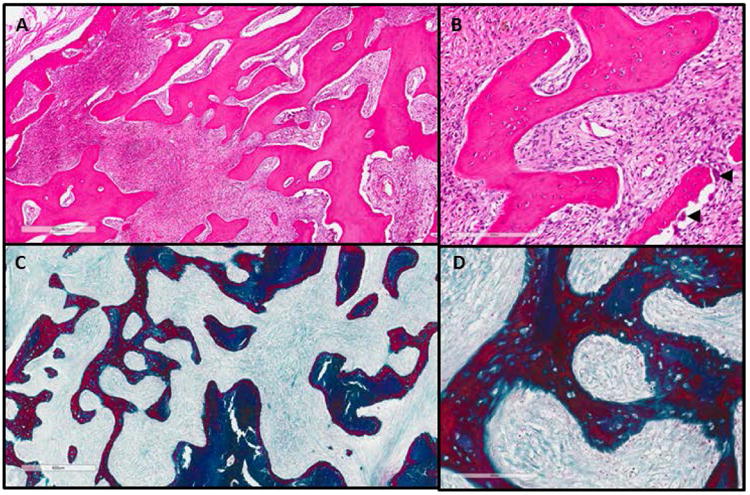
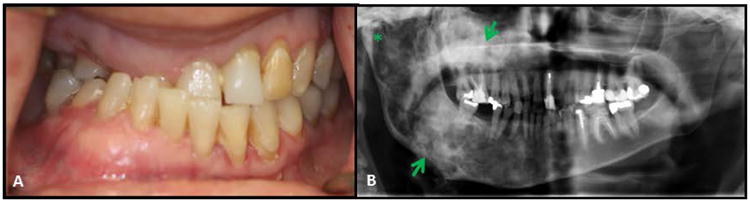
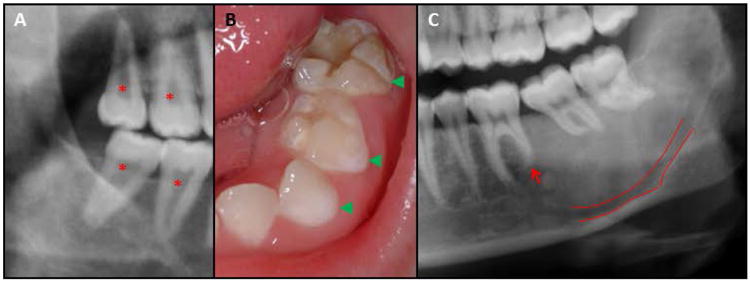
Fibrous dysplasia (FD) is a rare bone disease caused by postzygotic somatic activating mutations in the GNAS gene, which lead to constitutive activation of adenylyl cyclase and elevated levels of cyclic AMP, which act on downstream signaling pathways and cause normal bone to be replaced with fibrous tissue and abnormal (woven) bone. The bone disease may occur in one bone (monostotic), multiple bones (polyostotic), or in combination with hyperfunctioning endocrinopathies and hyperpigmented skin lesions (in the setting of McCune-Albright Syndrome). FD is common in the craniofacial skeleton, causing significant dysmorphic features, bone pain, and dental anomalies. This review summarizes the pathophysiology, clinical findings, and treatment of FD, with an emphasis on the craniofacial and oral manifestations of the disease.
Keywords: GNAS gene; McCune-Albright syndrome; craniofacial bone disease; dental anomalies; fibrous dysplasia.
Published 2016. This article is a U.S. Government work and is in the public domain in the USA.
Figures
Similar articles
-
Craniofacial Fibrous Dysplasia: Clinical and Therapeutic Implications.Curr Osteoporos Rep. 2023 Apr;21(2):147-153. doi: 10.1007/s11914-023-00779-6. Epub 2023 Feb 28. Curr Osteoporos Rep. 2023. PMID: 36849642 Free PMC article. Review.
-
Fibrous Dysplasia/McCune-Albright Syndrome: Clinical and Translational Perspectives.Curr Osteoporos Rep. 2016 Oct;14(5):178-86. doi: 10.1007/s11914-016-0317-0. Curr Osteoporos Rep. 2016. PMID: 27492469 Free PMC article. Review.
-
Extent of Extraskeletal Manifestations of Fibrous Dysplasia/McCune-Albright Syndrome in Patients with Mazabraud's Syndrome.Calcif Tissue Int. 2022 Mar;110(3):334-340. doi: 10.1007/s00223-021-00918-0. Epub 2021 Dec 2. Calcif Tissue Int. 2022. PMID: 34854944
-
[McCune-Albright syndrome: a case report and literature review].Pan Afr Med J. 2023 Sep 22;46:33. doi: 10.11604/pamj.2023.46.33.35274. eCollection 2023. Pan Afr Med J. 2023. PMID: 38145201 Free PMC article. Review. French.
-
[Pseudo precocious puberty in the McCune-Albright syndrome].Pediatrie. 1985 Jan-Feb;40(1):55-60. Pediatrie. 1985. PMID: 4022718 French.
Cited by
-
[Clinical guidelines «Precocious puberty»].Probl Endokrinol (Mosk). 2021 Sep 24;67(5):84-103. doi: 10.14341/probl12821. Probl Endokrinol (Mosk). 2021. PMID: 34766494 Free PMC article. Russian.
-
Comprehensive management of malocclusion in maxillary fibrous dysplasia: A case report.World J Clin Cases. 2021 Dec 6;9(34):10671-10680. doi: 10.12998/wjcc.v9.i34.10671. World J Clin Cases. 2021. PMID: 35005000 Free PMC article.
-
Multiscale molecular profiling of pathological bone resolves sexually dimorphic control of extracellular matrix composition.Dis Model Mech. 2021 Mar 1;14(3):dmm048116. doi: 10.1242/dmm.048116. Epub 2021 Mar 17. Dis Model Mech. 2021. PMID: 33563616 Free PMC article.
-
Fibrous Dysplasia of Bone and McCune-Albright Syndrome: A Bench to Bedside Review.Calcif Tissue Int. 2019 May;104(5):517-529. doi: 10.1007/s00223-019-00550-z. Epub 2019 Apr 29. Calcif Tissue Int. 2019. PMID: 31037426 Free PMC article. Review.
-
Navigation-assisted occipitocervical fixation and decompression in a patient with polyostotic fibrous dysplasia.J Craniovertebr Junction Spine. 2024 Jul-Sep;15(3):380-383. doi: 10.4103/jcvjs.jcvjs_104_24. Epub 2024 Sep 12. J Craniovertebr Junction Spine. 2024. PMID: 39483840 Free PMC article.
References
-
- Akintoye SO, Kelly MH, Brillante B, Cherman N, Turner S, Butman JA, Robey PG, Collins MT. Pegvisomant for the treatment of gsp-mediated growth hormone excess in patients with McCune-Albright syndrome. J Clin Endocrinol Metab. 2006;91:2960–6. - PubMed
-
- Akintoye SO, Lee JS, Feimster T, Booher S, Brahim J, Kingman A, Riminucci M, Robey PG, Collins MT. Dental characteristics of fibrous dysplasia and McCune-Albright syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:275–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
