

Assessing Risk in Patients with Stable Coronary Disease: When Should We Intensify Care and Follow-Up? Results from a Meta-Analysis of Observational Studies of the COURAGE and FAME Era
- PMID: 27239372
- PMCID: PMC4863126
- DOI: 10.1155/2016/3769152
Assessing Risk in Patients with Stable Coronary Disease: When Should We Intensify Care and Follow-Up? Results from a Meta-Analysis of Observational Studies of the COURAGE and FAME Era
Abstract
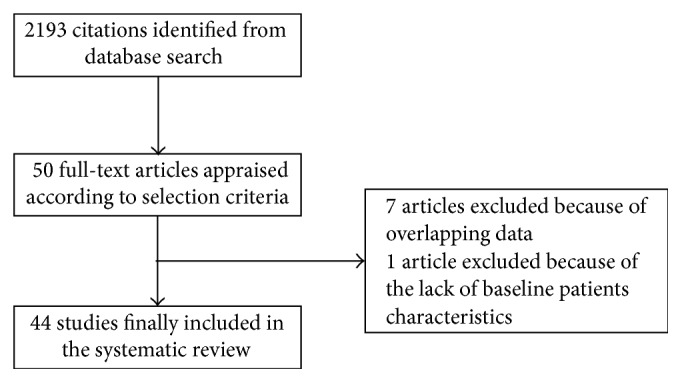
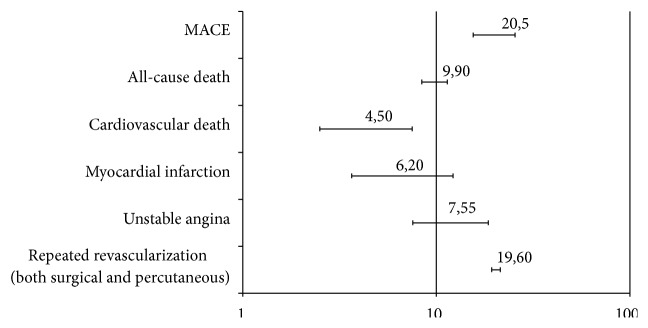
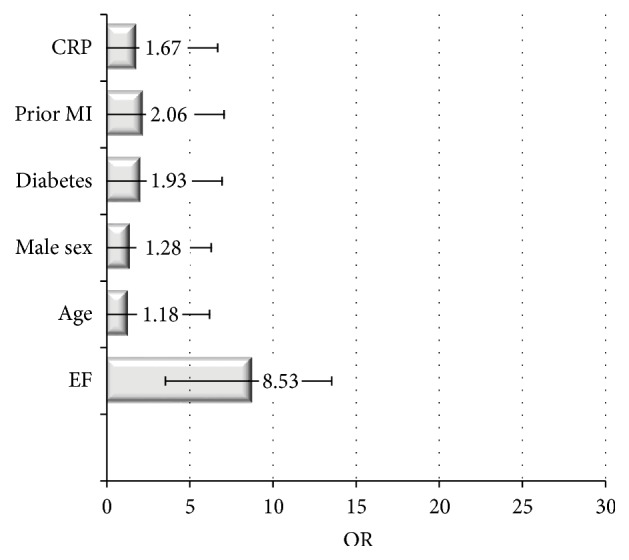
Background. A large number of clinical and laboratory markers have been appraised to predict prognosis in patients with stable angina, but uncertainty remains regarding which variables are the best predictors of prognosis. Therefore, we performed a meta-analysis of studies in patients with stable angina to assess which variables predict prognosis. Methods. MEDLINE and PubMed were searched for eligible studies published up to 2015, reporting multivariate predictors of major adverse cardiac events (MACE, a composite endpoint of death, myocardial infarction, and revascularization) in patients with stable angina. Study features, patient characteristics, and prevalence and predictors of such events were abstracted and pooled with random-effect methods (95% CIs). Major adverse cardiovascular event (MACE) was the primary endpoint. Results. 42 studies (104,559 patients) were included. After a median follow-up of 57 months, cardiovascular events occurred in 7.8% of patients with MI in 6.2% of patients and need for repeat revascularization (both surgical and percutaneous) in 19.5% of patients. Male sex, reduced EF, diabetes, prior MI, and high C-reactive protein were the most powerful predictors of cardiovascular events. Conclusions. We show that simple and low-cost clinical features may help clinicians in identifying the most appropriate diagnostic and therapeutic approaches within the broad range of outpatients presenting with stable coronary artery disease.
Figures

Similar articles
-
The relationship between revascularization extent and the long-term prognosis of patients with stable angina pectoris and three-vessel disease treated by percutaneous coronary intervention in the era of drug-eluting stents.Clin Cardiol. 2014 Sep;37(9):566-75. doi: 10.1002/clc.22309. Epub 2014 Aug 14. Clin Cardiol. 2014. PMID: 25123798 Free PMC article.
-
Exercise-based cardiac rehabilitation for coronary heart disease.Cochrane Database Syst Rev. 2016 Jan 5;2016(1):CD001800. doi: 10.1002/14651858.CD001800.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2021 Nov 6;11:CD001800. doi: 10.1002/14651858.CD001800.pub4. PMID: 26730878 Free PMC article. Updated. Review.
-
Prevalence of anginal symptoms and myocardial ischemia and their effect on clinical outcomes in outpatients with stable coronary artery disease: data from the International Observational CLARIFY Registry.JAMA Intern Med. 2014 Oct;174(10):1651-9. doi: 10.1001/jamainternmed.2014.3773. JAMA Intern Med. 2014. PMID: 25110899 Clinical Trial.
-
Heart failure with preserved ejection fraction: comparison of patients with and without angina pectoris (from the Duke Databank for Cardiovascular Disease).J Am Coll Cardiol. 2014 Jan 28;63(3):251-8. doi: 10.1016/j.jacc.2013.09.039. Epub 2013 Oct 23. J Am Coll Cardiol. 2014. PMID: 24161322 Free PMC article.
-
Treatment Strategies for Women With Coronary Artery Disease [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2012 Aug. Report No.: 12-EHC070-EF. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012 Aug. Report No.: 12-EHC070-EF. PMID: 23016160 Free Books & Documents. Review.
Cited by
-
Long term prognostic implication of newly detected abnormal glucose tolerance among patients with stable cardiovascular disease: a population-based cohort study.J Transl Med. 2021 Jun 30;19(1):277. doi: 10.1186/s12967-021-02950-y. J Transl Med. 2021. PMID: 34193200 Free PMC article.
-
The Influence of Cardiovascular Risk Factors and Hypogonadism on Cardiac Outcomes in an Aging Population of Beta-Thalassemia Patients.J Cardiovasc Dev Dis. 2021 Dec 21;9(1):3. doi: 10.3390/jcdd9010003. J Cardiovasc Dev Dis. 2021. PMID: 35050213 Free PMC article.
-
Incidence and risk factors for recurrent cardiovascular disease in middle-eastern adults: a retrospective study.BMC Cardiovasc Disord. 2019 Nov 11;19(1):253. doi: 10.1186/s12872-019-1231-z. BMC Cardiovasc Disord. 2019. PMID: 31711429 Free PMC article.
-
PR interval prolongation in coronary patients or risk equivalent: excess risk of ischemic stroke and vascular pathophysiological insights.BMC Cardiovasc Disord. 2017 Aug 24;17(1):233. doi: 10.1186/s12872-017-0667-2. BMC Cardiovasc Disord. 2017. PMID: 28836952 Free PMC article.
-
Risk factors for prehypertension and their interactive effect: a cross- sectional survey in China.BMC Cardiovasc Disord. 2018 Sep 15;18(1):182. doi: 10.1186/s12872-018-0917-y. BMC Cardiovasc Disord. 2018. PMID: 30219041 Free PMC article.
References
-
- Lim G. B. Global burden of cardiovascular disease. Nature Reviews Cardiology. 2013;10(2, article 59) - PubMed
-
- Daly C. A., De Stavola B., Sendon J. L., et al. Predicting prognosis in stable angina-results from the Euro heart survey of stable angina: prospective observational study. British Medical Journal. 2006;332:262–267. doi: 10.1136/bmj.38695.605440.ae. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
