

Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis
- PMID: 24863923
- PMCID: PMC4081236
- DOI: 10.1503/cmaj.140081
Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis
Abstract
Background: Mechanical ventilation in the prone position is used to improve oxygenation and to mitigate the harmful effects of mechanical ventilation in patients with acute respiratory distress syndrome (ARDS). We sought to determine the effect of prone positioning on mortality among patients with ARDS receiving protective lung ventilation.
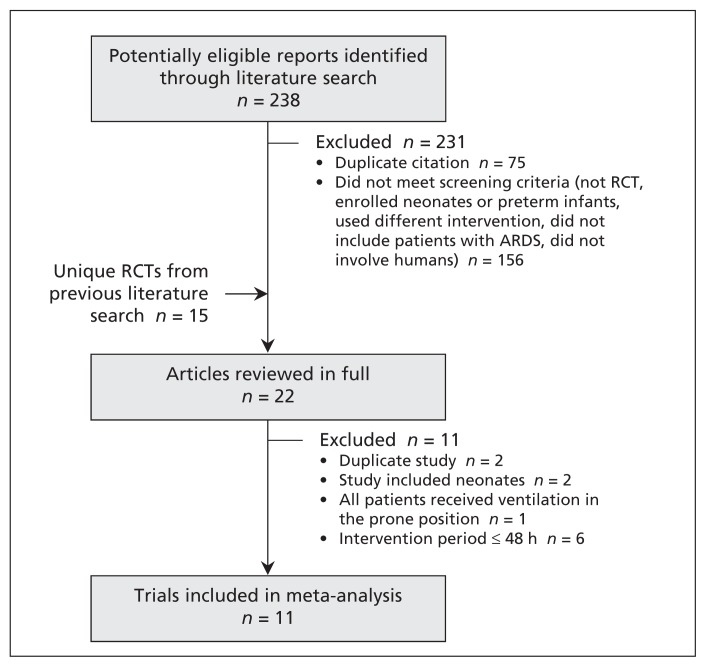
Methods: We searched electronic databases and conference proceedings to identify relevant randomized controlled trials (RCTs) published through August 2013. We included RCTs that compared prone and supine positioning during mechanical ventilation in patients with ARDS. We assessed risk of bias and obtained data on all-cause mortality (determined at hospital discharge or, if unavailable, after longest follow-up period). We used random-effects models for the pooled analyses.
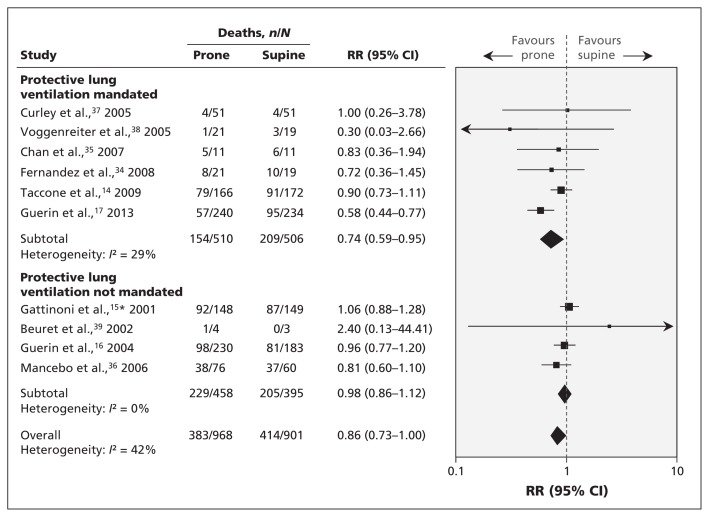
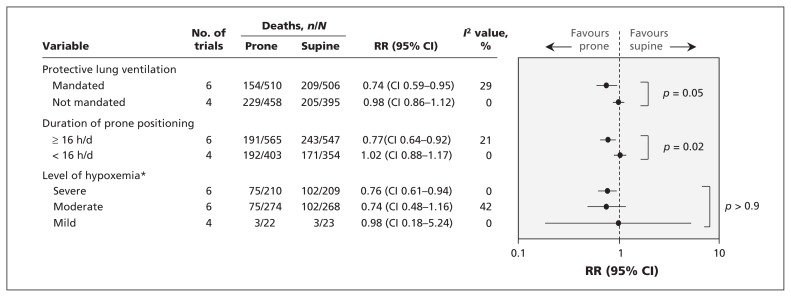
Results: We identified 11 RCTs (n=2341) that met our inclusion criteria. In the 6 trials (n=1016) that used a protective ventilation strategy with reduced tidal volumes, prone positioning significantly reduced mortality (risk ratio 0.74, 95% confidence interval 0.59-0.95; I2=29%) compared with supine positioning. The mortality benefit remained in several sensitivity analyses. The overall quality of evidence was high. The risk of bias was low in all of the trials except one, which was small. Statistical heterogeneity was low (I2<50%) for most of the clinical and physiologic outcomes.
Interpretation: Our analysis of high-quality evidence showed that use of the prone position during mechanical ventilation improved survival among patients with ARDS who received protective lung ventilation.
© 2014 Canadian Medical Association or its licensors.
Figures
Similar articles
-
Prone position for acute respiratory failure in adults.Cochrane Database Syst Rev. 2015 Nov 13;2015(11):CD008095. doi: 10.1002/14651858.CD008095.pub2. Cochrane Database Syst Rev. 2015. PMID: 26561745 Free PMC article. Review.
-
An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury.Crit Care. 2011;15(1):R6. doi: 10.1186/cc9403. Epub 2011 Jan 6. Crit Care. 2011. PMID: 21211010 Free PMC article.
-
Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis.CMAJ. 2008 Apr 22;178(9):1153-61. doi: 10.1503/cmaj.071802. CMAJ. 2008. PMID: 18427090 Free PMC article. Review.
-
Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta-analysis.Intensive Care Med. 2014 Mar;40(3):332-41. doi: 10.1007/s00134-013-3194-3. Epub 2014 Jan 17. Intensive Care Med. 2014. PMID: 24435203 Free PMC article.
-
Prone Position for Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2017 Oct;14(Supplement_4):S280-S288. doi: 10.1513/AnnalsATS.201704-343OT. Ann Am Thorac Soc. 2017. PMID: 29068269 Review.
Cited by
-
Severe community-acquired pneumonia: timely management measures in the first 24 hours.Crit Care. 2016 Aug 28;20(1):237. doi: 10.1186/s13054-016-1414-2. Crit Care. 2016. PMID: 27567896 Free PMC article. Review.
-
Optimal duration of prone positioning in patients with acute respiratory distress syndrome: a protocol for a systematic review and meta-regression analysis.BMJ Open. 2018 Sep 10;8(9):e021408. doi: 10.1136/bmjopen-2017-021408. BMJ Open. 2018. PMID: 30206081 Free PMC article.
-
Management of severe acute respiratory distress syndrome: a primer.Crit Care. 2023 Jul 18;27(1):289. doi: 10.1186/s13054-023-04572-w. Crit Care. 2023. PMID: 37464381 Free PMC article. Review.
-
Prone versus Supine Position Ventilation in Adult Patients with Acute Respiratory Distress Syndrome: A Meta-Analysis of Randomized Controlled Trials.Emerg Med Int. 2020 Nov 30;2020:4973878. doi: 10.1155/2020/4973878. eCollection 2020. Emerg Med Int. 2020. PMID: 33343939 Free PMC article.
-
Effect of Fu Zheng Jie Du Formula on outcomes in patients with severe pneumonia receiving prone ventilation: a retrospective cohort study.Front Pharmacol. 2024 Jul 24;15:1428817. doi: 10.3389/fphar.2024.1428817. eCollection 2024. Front Pharmacol. 2024. PMID: 39114366 Free PMC article.
References
-
- Ranieri VM, Suter PM, Tortorella C, et al. Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA 1999;282:54–61 - PubMed
-
- Dreyfuss D, Soler P, Basset G, et al. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis 1988;137:1159–64 - PubMed
-
- Muscedere JG, Mullen JB, Gan K, et al. Tidal ventilation at low airway pressures can augment lung injury. Am J Respir Crit Care Med 1994;149:1327–34 - PubMed
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:1301–8 - PubMed
-
- Briel M, Meade M, Mercat A, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA 2010;303:865–73 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous