

Mutations in the autoregulatory domain of β-tubulin 4a cause hereditary dystonia
- PMID: 23424103
- PMCID: PMC3698699
- DOI: 10.1002/ana.23832
Mutations in the autoregulatory domain of β-tubulin 4a cause hereditary dystonia
Abstract
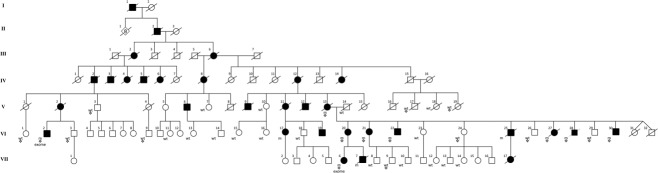
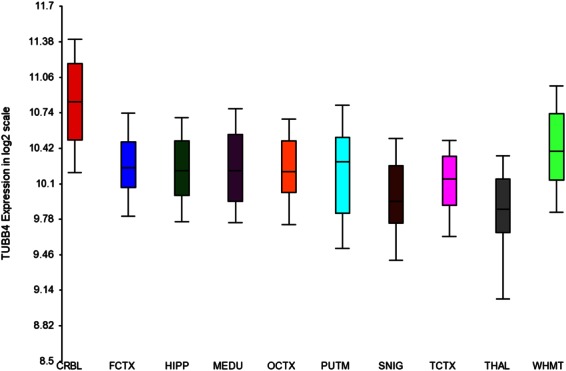
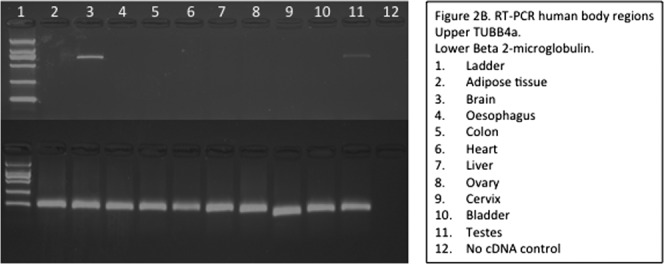
Dystonia type 4 (DYT4) was first described in a large family from Heacham in Norfolk with an autosomal dominantly inherited whispering dysphonia, generalized dystonia, and a characteristic hobby horse ataxic gait. We carried out a genetic linkage analysis in the extended DYT4 family that spanned 7 generations from England and Australia, revealing a single LOD score peak of 6.33 on chromosome 19p13.12-13. Exome sequencing in 2 cousins identified a single cosegregating mutation (p.R2G) in the β-tubulin 4a (TUBB4a) gene that was absent in a large number of controls. The mutation is highly conserved in the β-tubulin autoregulatory MREI (methionine-arginine-glutamic acid-isoleucine) domain, highly expressed in the central nervous system, and extensive in vitro work has previously demonstrated that substitutions at residue 2, specifically R2G, disrupt the autoregulatory capability of the wild-type β-tubulin peptide, affirming the role of the cytoskeleton in dystonia pathogenesis.
Copyright © 2012 American Neurological Association.
Figures
 ,
,  ,
,  ) indicates individuals included in linkage analysis. VI-27 and VI-28 were known to have Wilson disease and were also heterozygous for the R2G variant.
) indicates individuals included in linkage analysis. VI-27 and VI-28 were known to have Wilson disease and were also heterozygous for the R2G variant.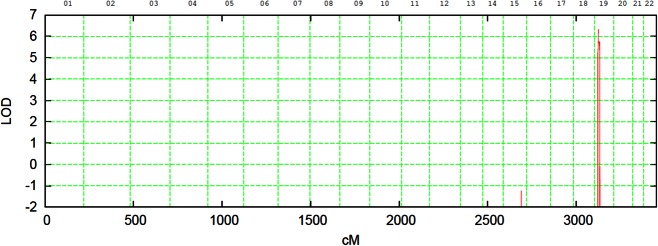

Similar articles
-
Pathogenic variants in TUBB4A are not found in primary dystonia.Neurology. 2014 Apr 8;82(14):1227-30. doi: 10.1212/WNL.0000000000000294. Epub 2014 Mar 5. Neurology. 2014. PMID: 24598712 Free PMC article.
-
Whispering dysphonia (DYT4 dystonia) is caused by a mutation in the TUBB4 gene.Ann Neurol. 2013 Apr;73(4):537-45. doi: 10.1002/ana.23829. Epub 2013 Apr 17. Ann Neurol. 2013. PMID: 23595291 Free PMC article.
-
DYT-TUBB4A (DYT4 Dystonia): New Clinical and Genetic Observations.Neurology. 2021 Apr 6;96(14):e1887-e1897. doi: 10.1212/WNL.0000000000010882. Epub 2020 Sep 17. Neurology. 2021. PMID: 32943487 Free PMC article.
-
Genotype-phenotype correlations in THAP1 dystonia: molecular foundations and description of new cases.Parkinsonism Relat Disord. 2012 Jun;18(5):414-25. doi: 10.1016/j.parkreldis.2012.02.001. Epub 2012 Feb 28. Parkinsonism Relat Disord. 2012. PMID: 22377579 Free PMC article. Review.
-
[A report of atypical hypomyelinating leukodystrophy with atrophy of the basal ganglia and cerebellum caused by a de novo mutation in tubulin beta 4A (TUBB4A) gene and literature review].Zhonghua Nei Ke Za Zhi. 2017 Jun 1;56(6):433-437. doi: 10.3760/cma.j.issn.0578-1426.2017.06.009. Zhonghua Nei Ke Za Zhi. 2017. PMID: 28592043 Review. Chinese.
Cited by
-
4EHP and GIGYF1/2 Mediate Translation-Coupled Messenger RNA Decay.Cell Rep. 2020 Oct 13;33(2):108262. doi: 10.1016/j.celrep.2020.108262. Cell Rep. 2020. PMID: 33053355 Free PMC article.
-
A de novo mutation in the β-tubulin gene TUBB4A results in the leukoencephalopathy hypomyelination with atrophy of the basal ganglia and cerebellum.Am J Hum Genet. 2013 May 2;92(5):767-73. doi: 10.1016/j.ajhg.2013.03.018. Epub 2013 Apr 11. Am J Hum Genet. 2013. PMID: 23582646 Free PMC article.
-
tubg1 Somatic Mutants Show Tubulinopathy-Associated Neurodevelopmental Phenotypes in a Zebrafish Model.Mol Neurobiol. 2025 Mar;62(3):3024-3039. doi: 10.1007/s12035-024-04448-2. Epub 2024 Aug 31. Mol Neurobiol. 2025. PMID: 39215931
-
A dominant tubulin mutation causes cerebellar neurodegeneration in a genetic model of tubulinopathy.Sci Adv. 2022 Feb 18;8(7):eabf7262. doi: 10.1126/sciadv.abf7262. Epub 2022 Feb 16. Sci Adv. 2022. PMID: 35171680 Free PMC article.
-
Dystonia Diagnosis: Clinical Neurophysiology and Genetics.J Clin Med. 2022 Jul 19;11(14):4184. doi: 10.3390/jcm11144184. J Clin Med. 2022. PMID: 35887948 Free PMC article. Review.
References
-
- Fahn S, Bressman SB, Marsden CD. Classification of dystonia. Adv Neurol. 1998;78:1–10. - PubMed
-
- Groen JL, Kallen MC, van de Warrenburg BP, et al. Phenotypes and genetic architecture of focal primary torsion dystonia. J Neurol Neurosurg Psychiatry. 2012;83:1006–1011. - PubMed
-
- Albanese A, Bentivoglio AR, Del Grosso N, et al. Phenotype variability of dystonia in monozygotic twins. J Neurol. 2000;247:148–150. - PubMed
-
- Albanese A, Lalli S. Update on dystonia. Curr Opin Neurol. 2012;25:483–490. - PubMed
-
- Phukan J, Albanese A, Gasser T, Warner T. Primary dystonia and dystonia-plus syndromes: clinical characteristics, diagnosis, and pathogenesis. Lancet Neurol. 2011;10:1074–1085. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- G0802462/MRC_/Medical Research Council/United Kingdom
- 089698/WT_/Wellcome Trust/United Kingdom
- MC_G0901330/MRC_/Medical Research Council/United Kingdom
- MR/J004758/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_09003/MRC_/Medical Research Council/United Kingdom
- G0802760/MRC_/Medical Research Council/United Kingdom
- G1001253/MRC_/Medical Research Council/United Kingdom
- G108/638/MRC_/Medical Research Council/United Kingdom
- G-0907/PUK_/Parkinson's UK/United Kingdom
- G-1107/PUK_/Parkinson's UK/United Kingdom
- MC_G1000735/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
