

Genetic defects in bile acid conjugation cause fat-soluble vitamin deficiency
- PMID: 23415802
- PMCID: PMC4175397
- DOI: 10.1053/j.gastro.2013.02.004
Genetic defects in bile acid conjugation cause fat-soluble vitamin deficiency
Abstract
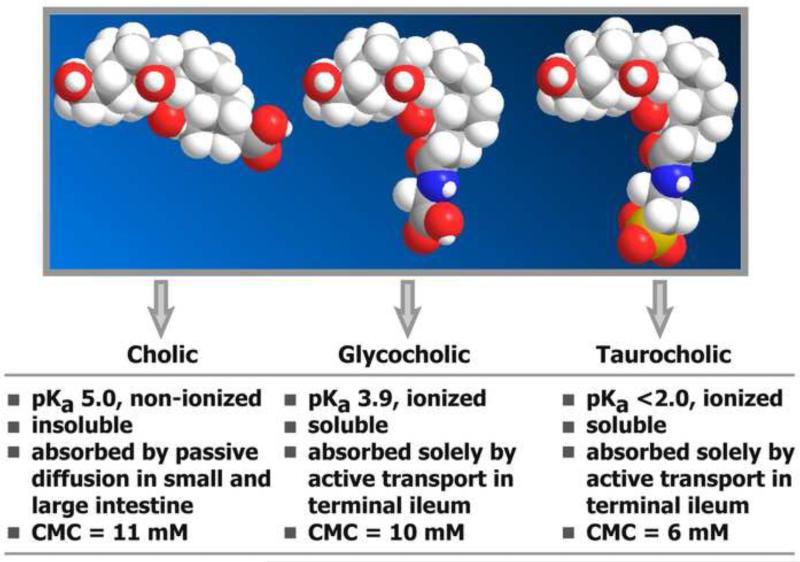
Background & aims: The final step in bile acid synthesis involves conjugation with glycine and taurine, which promotes a high intraluminal micellar concentration to facilitate lipid absorption. We investigated the clinical, biochemical, molecular, and morphologic features of a genetic defect in bile acid conjugation in 10 pediatric patients with fat-soluble vitamin deficiency, some with growth failure or transient neonatal cholestatic hepatitis.
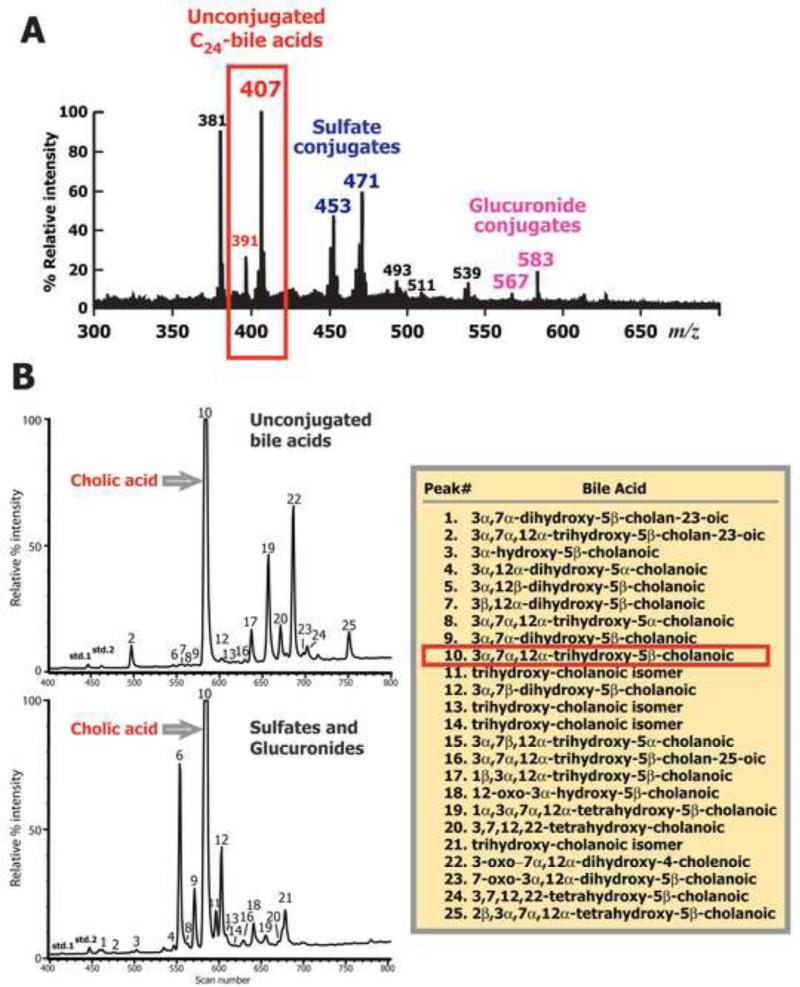
Methods: We identified the genetic defect that causes this disorder using mass spectrometry analysis of urine, bile, and serum samples and sequence analysis of the genes encoding bile acid-CoA:amino acid N-acyltransferase (BAAT) and bile acid-CoA ligase (SLC27A5).
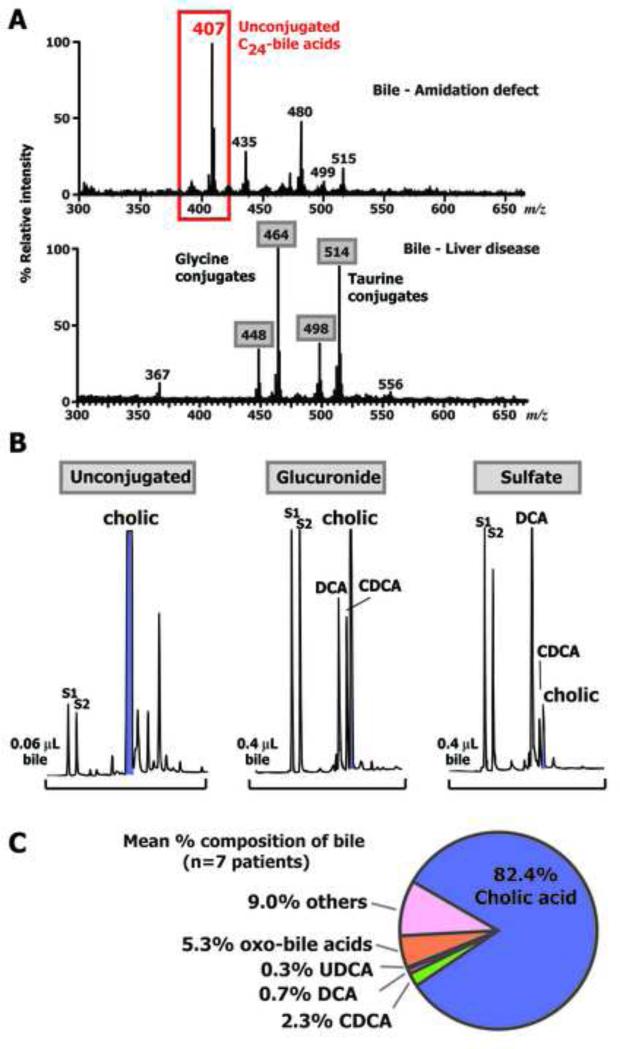
Results: Levels of urinary bile acids were increased (432 ± 248 μmol/L) and predominantly excreted in unconjugated forms (79.4% ± 3.9%) and as sulfates and glucuronides. Glycine or taurine conjugates were absent in the urine, bile, and serum. Unconjugated bile acids accounted for 95.7% ± 5.8% of the bile acids in duodenal bile, with cholic acid accounting for 82.4% ± 5.5% of the total. Duodenal bile acid concentrations were 12.1 ± 5.9 mmol/L, which is too low for efficient lipid absorption. The biochemical profile was consistent with defective bile acid amidation. Molecular analysis of BAAT confirmed 4 different homozygous mutations in 8 patients tested.
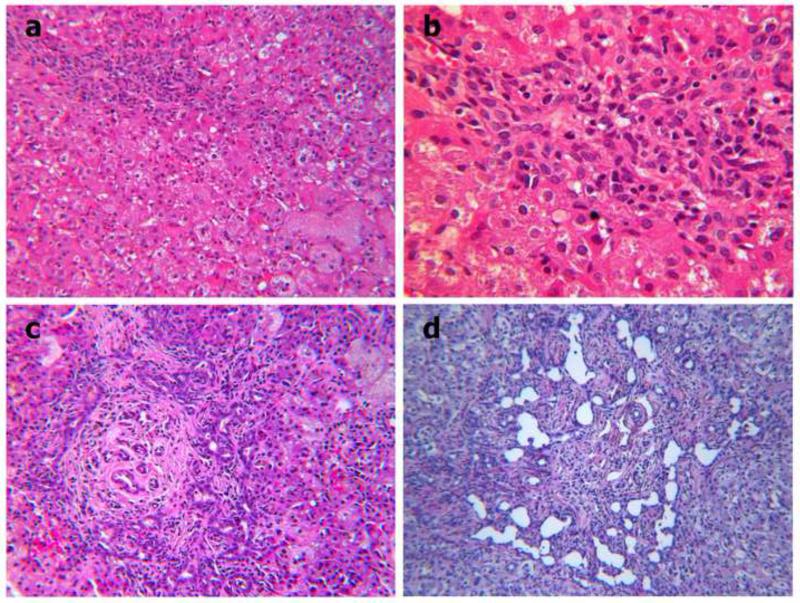
Conclusions: Based on a study of 10 pediatric patients, genetic defects that disrupt bile acid amidation cause fat-soluble vitamin deficiency and growth failure, indicating the importance of bile acid conjugation in lipid absorption. Some patients developed liver disease with features of a cholangiopathy. These findings indicate that patients with idiopathic neonatal cholestasis or later onset of unexplained fat-soluble vitamin deficiency should be screened for defects in bile acid conjugation.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
When bile acids don't get amidated.Gastroenterology. 2013 May;144(5):870-3. doi: 10.1053/j.gastro.2013.03.018. Epub 2013 Mar 22. Gastroenterology. 2013. PMID: 23523838 No abstract available.
Similar articles
-
Treatment of bile acid amidation defects with glycocholic acid.Hepatology. 2015 Jan;61(1):268-74. doi: 10.1002/hep.27401. Epub 2014 Dec 23. Hepatology. 2015. PMID: 25163551 Free PMC article.
-
Diagnosis in bile acid-CoA: amino acid N-acyltransferase deficiency.World J Gastroenterol. 2012 Jul 7;18(25):3322-6. doi: 10.3748/wjg.v18.i25.3322. World J Gastroenterol. 2012. PMID: 22783059 Free PMC article.
-
Bile acid-CoA ligase deficiency--a new inborn error of bile acid metabolism.J Inherit Metab Dis. 2012 May;35(3):521-30. doi: 10.1007/s10545-011-9416-3. Epub 2011 Nov 17. J Inherit Metab Dis. 2012. PMID: 22089923
-
[Infant with 3β-hydroxy-Δ(5)-C27 steroid dehydrogenase deficiency: report of two cases and literatures review].Zhonghua Er Ke Za Zhi. 2015 May;53(5):360-5. Zhonghua Er Ke Za Zhi. 2015. PMID: 26080666 Review. Chinese.
-
Inborn errors of bile acid metabolism in Japan.Pediatr Int. 2023 Jan;65(1):e15490. doi: 10.1111/ped.15490. Pediatr Int. 2023. PMID: 36704863 Review.
Cited by
-
Treatment of bile acid amidation defects with glycocholic acid.Hepatology. 2015 Jan;61(1):268-74. doi: 10.1002/hep.27401. Epub 2014 Dec 23. Hepatology. 2015. PMID: 25163551 Free PMC article.
-
Impact of Liver Inflammation on Bile Acid Side Chain Shortening and Amidation.Cells. 2022 Dec 9;11(24):3983. doi: 10.3390/cells11243983. Cells. 2022. PMID: 36552746 Free PMC article.
-
Deletion of hepatocyte cysteine dioxygenase type 1, a bile acid repressed gene, enhances glutathione synthesis and ameliorates acetaminophen hepatotoxicity.Biochem Pharmacol. 2024 Apr;222:116103. doi: 10.1016/j.bcp.2024.116103. Epub 2024 Feb 28. Biochem Pharmacol. 2024. PMID: 38428825
-
Bile acid receptors link nutrient sensing to metabolic regulation.Liver Res. 2017 Jun;1(1):17-25. doi: 10.1016/j.livres.2017.04.001. Epub 2017 Apr 26. Liver Res. 2017. PMID: 29098111 Free PMC article.
-
Loss of SLC27A5 Activates Hepatic Stellate Cells and Promotes Liver Fibrosis via Unconjugated Cholic Acid.Adv Sci (Weinh). 2024 Jan;11(2):e2304408. doi: 10.1002/advs.202304408. Epub 2023 Nov 13. Adv Sci (Weinh). 2024. PMID: 37957540 Free PMC article.
References
-
- Sjövall J. Dietary glycine and taurine conjugation in man. Proc Soc Exp Biol Med. 1959;100:676–8. - PubMed
-
- Matoba N, Une M, Hoshita T. Identification of unconjugated bile acids in human bile. J Lipid Res. 1986;27:1154–62. - PubMed
-
- Hofmann AF, Roda A. Physicochemical properties of bile acids and their relationship to biological properties: an overview of the problem. J Lipid Res. 1984;25:1477–89. - PubMed
-
- Killenberg PG. Measurement and subcellular distribution of choloyl-CoA synthetase and bile acid-CoA:amino acid N-acyltransferase activities in rat liver. J Lipid Res. 1978;19:24–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
