

Evidence of an asymmetrical endophenotype in congenital fibrosis of extraocular muscles type 3 resulting from TUBB3 mutations
- PMID: 20393110
- PMCID: PMC2941178
- DOI: 10.1167/iovs.10-5438
Evidence of an asymmetrical endophenotype in congenital fibrosis of extraocular muscles type 3 resulting from TUBB3 mutations
Abstract
Purpose: Orbital magnetic resonance imaging (MRI) was used to investigate the structural basis of motility abnormalities in congenital fibrosis of the extraocular muscles type 3 (CFEOM3), a disorder resulting from missense mutations in TUBB3, which encodes neuron-specific beta-tubulin isotype III.
Methods: Ophthalmic examinations in 13 volunteers from four CFEOM3 pedigrees and normal control subjects, were correlated with TUBB3 mutation and MRI findings that demonstrated extraocular muscle (EOM) size, location, contractility, and innervation.
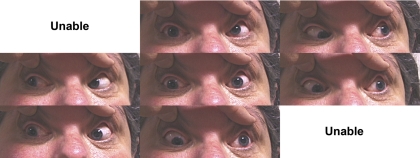
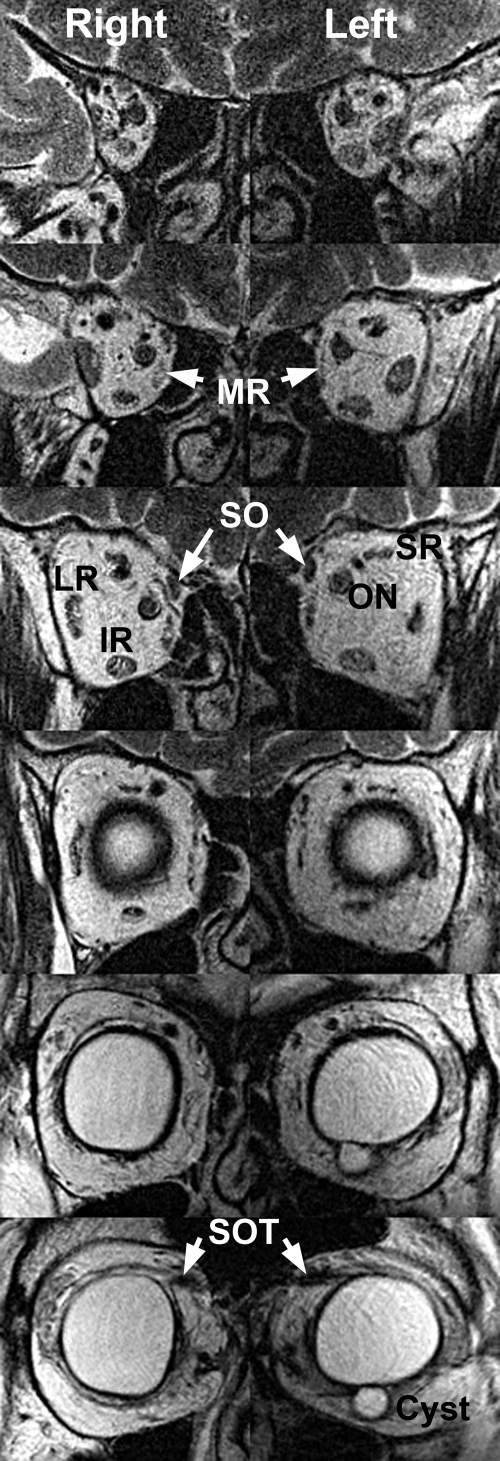
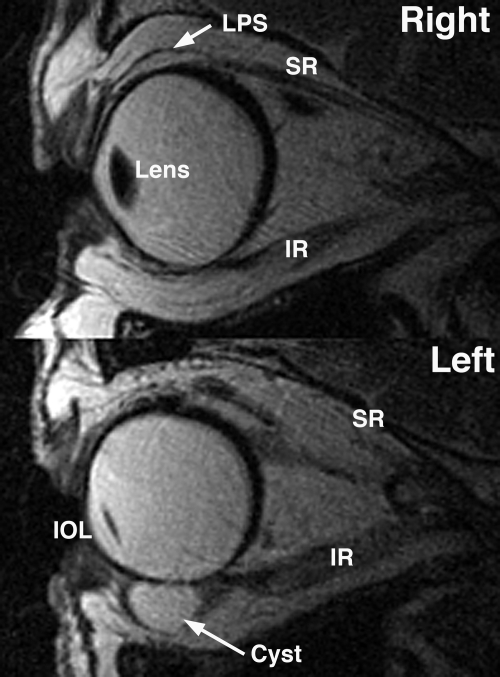
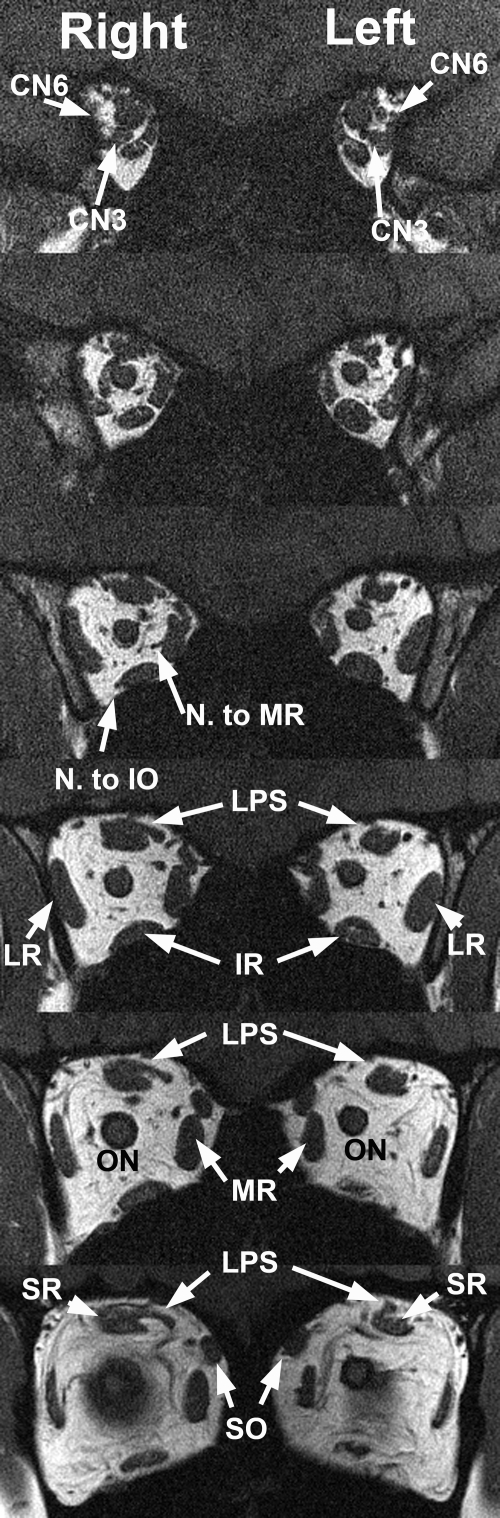
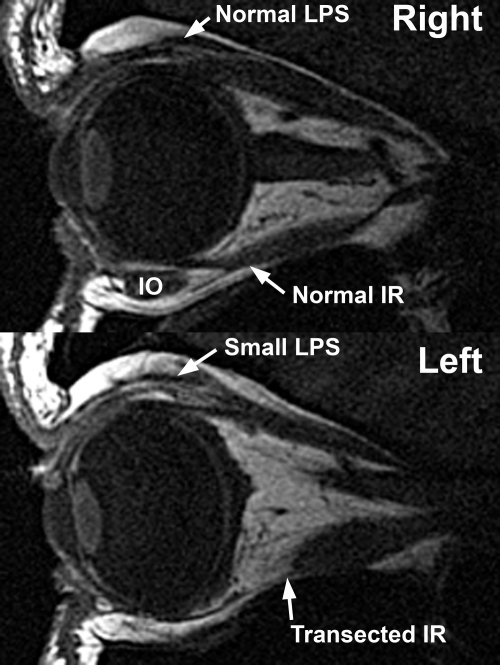
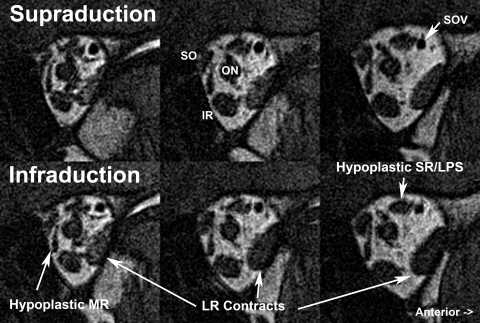
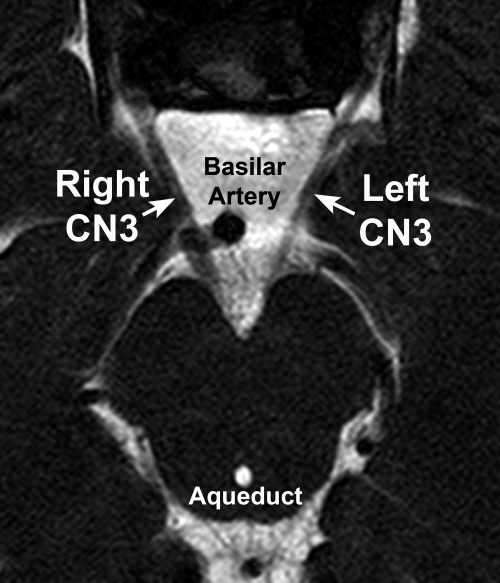
Results: Volunteers included clinically affected and clinically unaffected carriers of R262C and D417N TUBB3 amino acid substitutions and one unaffected, mutation-negative family member. Subjects with CFEOM3 frequently had asymmetrical blepharoptosis, limited vertical duction, variable ophthalmoplegia, exotropia, and paradoxical abduction in infraduction. MRI demonstrated variable, asymmetrical levator palpebrae superioris and superior rectus EOM atrophy that correlated with blepharoptosis, deficient supraduction, and small orbital motor nerves. Additional EOMs exhibited variable hypoplasia that correlated with duction deficit, but the superior oblique muscle was spared. Ophthalmoplegia occurred only when the subarachnoid width of CN3 was <1.9 mm. A-pattern exotropia was frequent, correlating with apparent lateral rectus (LR) muscle misinnervation by CN3. Optic nerve (ON) cross sections were subnormal, but rectus pulley locations were normal.
Conclusions: CFEOM3 caused by TUBB3 R262C and D417N amino acid substitutions features abnormalities of EOM innervation and function that correlate with subarachnoid CN3 hypoplasia, occasional abducens nerve hypoplasia, and subclinical ON hypoplasia that can resemble CFEOM1. Clinical and MRI findings in CFEOM3 are more variable than those in CFEOM1 and are often asymmetrical. Apparent LR innervation by the inferior rectus motor nerve is an overlapping feature of Duane retraction syndrome and CFEOM1. These findings suggest that CFEOM3 is an asymmetrical, variably penetrant, congenital cranial dysinnervation disorder leading to secondary EOM atrophy.
Figures



Similar articles
-
Ocular congenital cranial dysinnervation disorders (CCDDs): insights into axon growth and guidance.Hum Mol Genet. 2017 Aug 1;26(R1):R37-R44. doi: 10.1093/hmg/ddx168. Hum Mol Genet. 2017. PMID: 28459979 Free PMC article. Review.
-
Magnetic resonance imaging evidence for widespread orbital dysinnervation in congenital fibrosis of extraocular muscles due to mutations in KIF21A.Invest Ophthalmol Vis Sci. 2005 Feb;46(2):530-9. doi: 10.1167/iovs.04-1125. Invest Ophthalmol Vis Sci. 2005. PMID: 15671279
-
Magnetic resonance imaging of innervational and extraocular muscle abnormalities in Duane-radial ray syndrome.Invest Ophthalmol Vis Sci. 2007 Dec;48(12):5505-11. doi: 10.1167/iovs.07-0772. Invest Ophthalmol Vis Sci. 2007. PMID: 18055799 Free PMC article.
-
Magnetic resonance imaging evidence for widespread orbital dysinnervation in dominant Duane's retraction syndrome linked to the DURS2 locus.Invest Ophthalmol Vis Sci. 2007 Jan;48(1):194-202. doi: 10.1167/iovs.06-0632. Invest Ophthalmol Vis Sci. 2007. PMID: 17197533 Free PMC article.
-
Imaging of congenital cranial dysinnervation disorders: What radiologist wants to know?Clin Imaging. 2021 Mar;71:106-116. doi: 10.1016/j.clinimag.2020.10.055. Epub 2020 Nov 6. Clin Imaging. 2021. PMID: 33189029 Review.
Cited by
-
Two novel CHN1 mutations in 2 families with Duane retraction syndrome.Arch Ophthalmol. 2011 May;129(5):649-52. doi: 10.1001/archophthalmol.2011.84. Arch Ophthalmol. 2011. PMID: 21555619 Free PMC article.
-
Ocular congenital cranial dysinnervation disorders (CCDDs): insights into axon growth and guidance.Hum Mol Genet. 2017 Aug 1;26(R1):R37-R44. doi: 10.1093/hmg/ddx168. Hum Mol Genet. 2017. PMID: 28459979 Free PMC article. Review.
-
A Mutation in the Tubulin-Encoding TUBB3 Gene Causes Complex Cortical Malformations and Unilateral Hypohidrosis.Child Neurol Open. 2016 Sep 1;3:2329048X16665758. doi: 10.1177/2329048X16665758. eCollection 2016 Jan-Dec. Child Neurol Open. 2016. PMID: 28503613 Free PMC article.
-
Functional magnetic resonance imaging of horizontal rectus muscles in esotropia.J AAPOS. 2013 Feb;17(1):16-21. doi: 10.1016/j.jaapos.2012.09.016. Epub 2013 Jan 24. J AAPOS. 2013. PMID: 23352382 Free PMC article.
-
Sclerosing cavernous hemangioma of the cavernous sinus mimicking congenital fibrosis of the extraocular muscles.J AAPOS. 2014 Jun;18(3):299-301. doi: 10.1016/j.jaapos.2014.02.006. Epub 2014 Apr 18. J AAPOS. 2014. PMID: 24751811 Free PMC article.
References
-
- Gutowski NJ, Bosley TM, Engle EC. The congenital cranial dysinnervation disorders (CCDDs). 110th ENMCC International Workshop, Naarden, The Netherlands, October, 25–27, 2002. Neuromusc Dis. 2003;13:573–578 - PubMed
-
- Engle EC, Goumnerov BC, McKeown CA, et al. Oculomotor nerve and muscle abnormalities in congenital fibrosis of the extraocular muscles. Ann Neurol. 1997;41:314–325 - PubMed
-
- Engle EC, Kunkel LM, Specht LA, Beggs AH. Mapping a gene for congenital fibrosis of the extraocular muscles to the centromeric region of chromosome 12. Nat Genet. 1994;7:69–73 - PubMed
-
- Yamada K, Andrews C, Chan W-M, et al. Heterozygous mutations of the kinesin KIF21A in congenital fibrosis of the extraocular muscles type 1 (CFEOM1). Nat Genet. 2003;35:318–321 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 EY008313-20/EY/NEI NIH HHS/United States
- EY08313/EY/NEI NIH HHS/United States
- R01 EY012498/EY/NEI NIH HHS/United States
- R01 EY008313-19/EY/NEI NIH HHS/United States
- EY12498/EY/NEI NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- R01 EY008313-18/EY/NEI NIH HHS/United States
- R01 EY013583/EY/NEI NIH HHS/United States
- P30 EY000331/EY/NEI NIH HHS/United States
- EY00331/EY/NEI NIH HHS/United States
- EY13583/EY/NEI NIH HHS/United States
- T32 EY007143/EY/NEI NIH HHS/United States
- R01 EY008313/EY/NEI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
